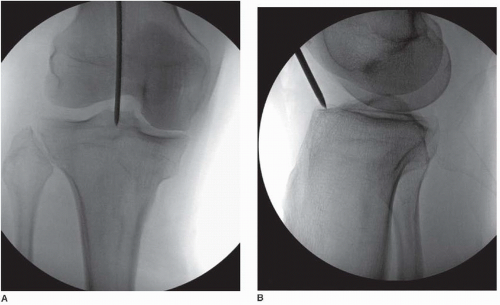
A 15-year-old male with osteogenesis imperfecta sustained a left tibial shaft fracture. We performed open reduction and intramedullary interlocking nailing (IMIL nail 8 mm). Intraoperatively, we encountered multiple iatrogenic fractures and longitudinal splits due to the brittle nature of OI bone. On postoperative review, the entry point appeared slightly lateral and distal compared to the ideal location, and the nail size may have been larger than optimal.
Let us discuss about some learnings from this case:
Surgical fixation for long bone fractures is indicated at a younger age in OI patients than in normal population, because it facilitates early mobilization and prolonged protection. The author of a paper did not hesitate to perform surgical fixation for a femoral or tibial shaft fracture after 3 years of age. Preexisting angular deformity predisposes a long bone to recurrent fractures. Hence, if surgical fixation is attempted, the preexisting deformity should be corrected simultaneously.
Fixation Options for Fracture/Osteotomy in OI
- General Principle: Fixators should minimize stress risers and ideally last until skeletal maturity.
- Plate and Screws:
- Can achieve union but cause stress concentration at plate tips → high risk of peri-implant fractures.
- Use only when no other options are viable.
- Single/multiple screws without plates also increase stress; avoid if possible.
- Tension Bands:
- Suitable for small fragments at long bone ends (e.g., olecranon fractures, metaphyseal osteotomies).
- Use long intramedullary (IM) pins to reduce stress risers.
- Intramedullary (IM) Rods:
- Preferred fixation for long bones in OI because they:
- Distribute stress evenly, protect entire bone length, and prevent osteopenia.
- Flexible IM rods:
- Risk of rod tips cutting through osteopenic cortex and soft tissue irritation.
- Use only if cortex is thickened and bone is curved without straightening.
- Rigid, straight IM rods:
- Best choice after straightening long bones via multi-level osteotomies (Sofield procedure).
- Strengthens bone mechanically, prevents displacement, improves function.
- Preferred fixation for long bones in OI because they:
- Telescopic IM Rods:
- Developed to avoid outgrowing simple rods in growing children.
- Examples: Bailey-Dubow, Sheffield, Fassier-Duval, interlocking telescopic rods.
- Consist of a hollow sleeve and obturator anchored at epiphyses.
- Failures occur if telescoping stops or anchorage fails, leading to stress risers and fractures.
- Even with perfect rod placement, severe OI bones may deform and cause rod complications.
- External Fixators:
- Generally not recommended due to stress risers at pins and poor pin purchase.
- May be used temporarily for gradual correction of severe deformity, then converted to IM rod fixation ASAP.
- Acute correction with IM rod preferred due to better soft-tissue tolerance in OI.
- Limb lengthening possible in mild OI but risks poor bone regenerate and joint damage.
Augmenting Fixation
- OI patients typically heal well, but poor bone stock in adolescents/adults can impair fixation and union.
- Thin diaphyseal cortex limits IM rod size and fixation strength.
- Bisphosphonates may suppress remodeling and delay healing.
- Additional fixation techniques:
- Locking plates with unicortical screws around IM rod (remove after union).
- Sandwich technique with cortical allograft straps for bone stock augmentation (limited experience).
- Infection and bone devitalization risks must be considered.
Reference::: CIOS :: Clinics in Orthopedic Surgery
Important Considerations
1. Challenges of Tibial Nailing in OI
- Bone fragility → cortex thin, medullary canal narrow and irregular.
- Tendency to split longitudinally during reaming or nail insertion.
- Risk of iatrogenic fractures at entry site, along the shaft, or even in metaphyseal areas.
2. Entry point considerations in IM nailing of tibia
- Ideal: Centered just medial to the lateral tibial spine in the AP view, and at the anterior edge of the tibial plateau in the lateral view.
- Too lateral: Can cause eccentric reaming, cortical perforation, or asymmetric loading → increased fracture propagation risk.
- Too distal: Leads to posterior nail trajectory, increasing risk of fracture at the entry site or difficulty seating the nail.
In OI:
- The tolerance for even small deviations is reduced because the cortex is so thin and brittle.
- A lateral/distal start point increases hoop stresses during insertion → splits can propagate easily.
3. Nail size selection
Humeral Nail for Tibial Reconstruction in Adolescent OI (Indian J Orthop Surg, 2022):
- A case report demonstrates a successful alternative using a 6.5 mm interlocking humeral nail smaller and more anatomically compatible for tibial fixation in adolescent OI.
- Key advantages include:
- Better fit for narrow medullary canals
- Rotational stability and limb-length control, outperforming simple Rush pins
- Manageable outcomes even when cortical splits occur, with grafting as needed
An 8 mm nail in a 15-year-old OI tibia might be too stiff and large, especially if reaming caused microcracks or if cortical thickness was uneven.
Further reading: Humerus nail for tibial reconstruction in adolescent with osteogenesis imperfecta – A rare surgical case report – Indian J Orthop Surg

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.