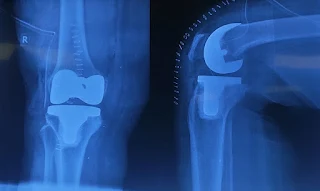
Recently, we operated on a 58-year-old female patient with advanced bilateral knee osteoarthritis (OA). She underwent simultaneous bilateral total knee arthroplasty (TKA) using a medial parapatellar approach. Both femoral components were size 3, tibial components size 3, and a 10mm polyethylene insert was used on each side.

Some practical considerations from our case:
1. We operated on the more symptomatic leg first
2. We prepared both the knees at the same time but positioned the second log with side-posts only before starting the surgery on that side
Potential advantages:
- Single anesthesia and hospital admission.
- Shorter overall recovery period compared to two separate procedures.
- Lower combined costs and reduced total inpatient days in some studies.
- Patient convenience – one rehab period instead of two.
Reported risks and concerns:
a. Mortality
- 2009 review: Reports mixed findings, with some studies showing no mortality difference, others showing higher risk.
- 2012 JBJS Br:
- Swedish Knee Arthroplasty Register: 7.53× higher 30-day mortality vs. second stage of staged procedure; 3.77× higher vs. unilateral TKA.
- Estimated 1.94× higher mortality vs. staged bilateral overall.
- Multiple meta-analyses (Restrepo et al., Hu et al.) confirm higher mortality risk.
b. Cardiac & Pulmonary Complications
- Higher incidence of myocardial infarction, pulmonary embolism, and neurological events after SBTKA (meta-analysis data).
- Increased fat embolism risk – though absolute rates are low (around 0.17%).
c. Other Medical Risks
- Higher rates of gastrointestinal complications (especially ileus).
- More frequent hemodynamic instability intraoperatively (hypotension/bradycardia).
d. Surgical Risks
- Greater perioperative blood loss and transfusion requirements, with transfusions independently linked to prosthetic joint infection and longer stays.
- Longer operative times, potentially increasing infection risk.
Cost considerations
- While SBTKA may reduce initial hospitalization costs, the need for acute rehabilitation care post-discharge can offset savings.
- Medicare and some insurance reimbursement policies reduce payment for the second knee in simultaneous procedures, discouraging use.
Patient Selection & Setting
- Strict selection criteria – younger, healthier patients without major cardiopulmonary comorbidities.
- Morbid obesity emerges as a distinct, high-risk factor demonstrating that SBTKA in this population notably increases operative and postoperative risks.
- High-volume centers with experience in SBTKA and access to advanced perioperative monitoring and intensive postoperative support.
- Consideration of two-team approach to reduce operative time.
References:
- Parvizi, J., & Rasouli, M. R. (2012). Simultaneous-bilateral TKA. The Journal of Bone and Joint Surgery. British Volume, 94-B(11_Supple_A), 90–92.
- Noble, J., Goodall, J. R., & Noble, D. J. (2009). Simultaneous Bilateral Total Knee Replacement: A persistent controversy. The Knee, 16(6), 420–426.
- Akar B. Is there an indication for simultaneous bilateral knee arthroplasty in morbidly obese patients? Should the patients’ request for simultaneous operation be considered? PLoS One. 2023 Oct 25;18(10):e0287021. doi: 10.1371/journal.pone.0287021. PMID: 37878579; PMCID: PMC10599534.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.