SIRS criteria are mostly used as a screening tool to identify patients that may need further workup for sepsis and severe sepsis. In the emergency department it is a triage tool that helps determine patient acuity and identify patients that are potentially septic and in need of further screening.
Septic shock is the most severe manifestation in a continuum.
- SIRS = Severe Inflammatory Response Syndrome
- Sepsis = SIRS + Known source of infection
- Severe Sepsis = Sepsis + Organ dysfunction, Hypoperfusion abnormalities or Hypotension
- Lactic Acidosis, SBP <90 or SBP Drop ≥ 40 mm Hg of normal
- Septic Shock = Sepsis induced hypotension refractory to fluid resuscitation and hypoperfusion abnormalities
- Multiple Organ Dysfunction Syndrome (MODS) = Evidence of ≥ 2 Organs Failing
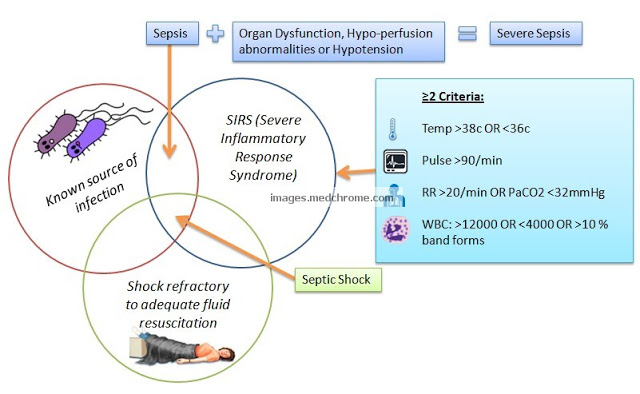
Consensus conference definition for SIRS:
- Temperature > 38°C or < 36°C
- Heart rate > 90 beats/minute
- Respiration > 20/min or PaCO2 < 32mm Hg
- Leukocyte count > 12,000/mm3, < 4,000/mm3 or > 10% immature (band) cells
The SIRS criteria for pediatric patients is age group dependent.
Hypoperfusion abnormalities:
- Lactic acidosis
- Oliguria
- Or an acute alteration in mental status
Organ Dysfunctions:
- Lungs: Early fall in PO2, ARDS, capillary leakage into alveoli, tachypnea, hyperpnea
- Kidneys: ARF (oliguira, anuria, azotemia, proteinuria)
- Liver: Elevated serum bilirubin, ALP, cholestatic jaundice
- GIT: Nausea, vomiting, diarrhea and ileus
- Skin: Ecthyma gangrenosum, petechia or purpura, hemorrhage or bullous lesions, generalized erythroderma
- Heart: Cardiac output is initially elevated or normal
- Brain: Confusion
Common surgical causes of SIRS:
- Acute pancreatitis
- Perforated viscus with peritonitis
- Fulminant hepatitis
- Multiple trauma
- Massive blood transfusion
- Aspiration pneumonia
- Ischemic reperfusion injury
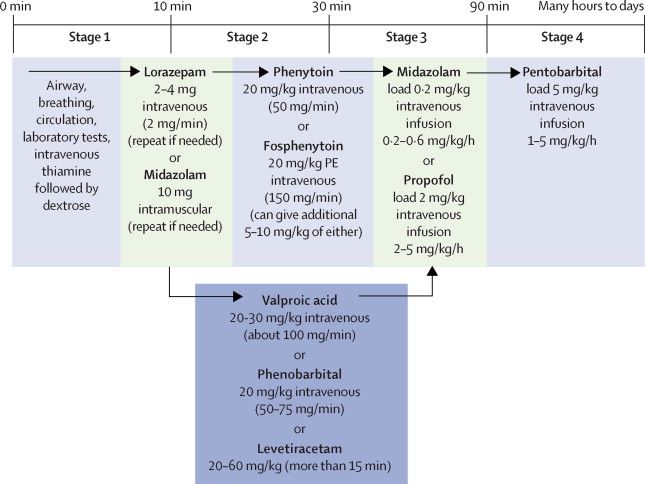
Management:
Initiate within the first 6 hours of resuscitation upon initial recognition for adults and within 60 minutes upon initial recognition for pediatric patients.
- Serum lactate: within 3 hours of presentation
- Blood Cultures: prior to antibiotics
- Empiric broad-spectrum antibiotics (Later based on culture and sensitivity)
- Initial fluid administration:
- Adults: 30 ml/kg crystalloid or colloid equivalent for hypotension or lactate >4 mmol/L
- Children: 20 ml/kg crystalloid in children
- Vasopressor: for persistent hypotension (MAP <65 in adults) despite initial fluid administration.
- Re-measure lactate if the initial value was elevated.
- CVP measurement: In a severely septic/septic shock patient in the first 6 hours after presentation if ≥1 of the following met:
- Persistent hypotension despite fluid resuscitation
- Requires vasopressor therapy
- Inability to obtain adequate peripheral vascular access
Contraindications to the above:
1. Patient is at risk for bleeding
2. Patient is too unstable/code imminent
3. Patient has a high risk of developing pneumothorax
4. Insertion of line would not change the course of treatment
5. Patient refuses to give consent
6. Vascular access is not possible (e.g., bilateral clots)
Reference: Surviving Sepsis Campaign
Note: SIRS criteria is no more used to define Sepsis and Septic shock.