Views
- Standard: Supine AP and Latero-lateral (LL) views – thoracic or lumbar
- Thoracic:
- Lateral (Fulcrum) bending views: to determine the flexibility of curves in scoliosis
- Lumbar:
- De Seze view (Lumbopelvic view): Standing AP and LL – shows T11 to head of femur
- Dynamic lateral (flexion-extension) views: for instability
- Oblique views (45 degrees): better delineation of pars interarticularis and facet joints
- Lumbosacral:
- Ferguson view: 20 degrees caudocephalic AP view of lumbosacral joint – for farout syndrome (5th root compression produced by a large transverse process of L5 against sacral ala)
- Whole spine imaging: when alignment of spine, sagittal and coronal balance, and pelvic parameters are to be assessed

Detecting the correct level
- Highest point on the iliac crest usually points to L4/5 on the lateral view
- Count from C2 downwards if you have full spine X-ray
- The 12th rib can be helpful
If confusion still exists between sacralization of L5 and lumbarization of S1, then it would be safe to comment on pathology based on the last mobile level. This is the level that has no bony connection to the pelvis, such as the large transverse process articulating with the ilium. This is usually the level where disc degeneration occurs.
On Both AP and Lateral views
- Vertebral bodies and spinous processes must be aligned in normal line of curvatures.
- Height of vertebral bodies should be equal.
- Width of intervertebral disc spaces should be uniform.
- Continuity of superior and inferior endplates should remain unbroken.
- Distance between spinous process should be equal.
- Trace the posterior elements; the pedicles, laminae, and spinous processes.
On AP view
Normal vertebra in AP view can be assumed as an owl with pedicles representing the eyes, spinous process representing the beak, vertebral bodies representing the head and transverse process or transverse process-rib complex as the wings.
Congenital pathology:
- Butterfly vertebra: Failure of fusion of 2 lateral halves of vertebra due to persistent notochordal tissue
- Hemivertebra: Only 1 side of vertebra develops
- Non-segmented: not separated from level above or below
- Fully segmented (free): not attached to level above or below
- Semi segmented: half vertebra is fused with level above or below
- Incarcerated: joined by pedicles to segment above or below
- Unilateral bar vertebra +/- contralateral hemivertebra: failure of segmentation on 1 side
- Block vertebra: failure of segmentation on both sides
- Transitional vertebra: Bertolloti syndrome (transitional vertebra + low back pain)
- Sacralization of L5: L5 is fused to sacrum
- Lumbarization of S1: S1 is detached from sacrum
- Spina bifida: Failure of fusion of neural arch (can be seen as defect in fusion around the spinous process)
Traumatic pathology:
- Compression fractures: Decreased vertebral height
- Unstable burst fractures: Widening of interpedicular distance
- Chance fractures: Horizontal fracture through the pedicles; Widening of interspinous space (empty vertebra sign)
- Paravertebral hematoma: Widening of paravertebral lines
Degenerative pathology:
- Facet joints: In lumbar spine, best viewed in oblique views
- Joint space narrowing, subchondral cysts and/or sclerosis, vacuum phenomenon and osteophyte formation
- Intervertebral disc:
- Osteochondrosis – Narrowing of intervertebral disc space, central vacuum phenomenon, sclerosis of vertebral endplates and subchondral bone, and asymmetric osteophytes in any direction
- Spondylosis deformans – symmetrical anterolateral osteophytes, preservation or mild reduction of disc space, peripheral vacuum phenomenon, sclerosis and/or amputation of epiphyseal ring
- Ligaments and their insertions into bone (DISH):
- Presence of large bridging osteophytes in atleast 4 adjacent thoracic vertebrae
- Congenital spinal stenosis (seen more frequently in lumbar tract):
- Lowering or absence of increase in Interpedicular distance from L1 (normally 17-19 mm) to L5 (normally 20-23 mm)
- Central spinal stenosis: Canal to body ratio < 1 : 4.5
- [Interpedicular distance in AP view X Spinal canal distance in lateral view]/[Width of vertebral body in AP view X Width of vertebral body in lateral view]
Vacuum phenomena involving the intervertebral discs is usually a result of an accumulation of gas, principally nitrogen, within the crevices of the intervertebral discs or adjacent vertebrae.
Spondylolisthesis:
Inverted napolean hat sign: Frontal orientation of the brim of the upper endplate and the transverse processes of L5 can project an image called “the inverted Napoleon hat” sign
Seronegative spondyloarthropathy:
Ankylosing spondylitis and inflammatory bowel disease tend to show symmetric bilateral involvement, psoriatic and reactive spondyloarthropathy tend to be coarser and more asymmetrical.
New York Sacroiliitis grading:
- 0 – Normal
- 1 – Suspicious change
- 2 – Minimum abnormality (small localized areas with erosion or sclerosis, without alteration in the joint width)
- 3 – Unequivocal abnormality (moderate or advanced sacroiliitis with erosions, evidence of sclerosis, widening, narrowing, or partial ankyloses)
- 4 – Severe abnormality (total ankyloses)
Ankylosing spondylitis:
- Syndesmophyte: Vertical bone bridges
- Dagger sign: A hyperdense line along the central spine secondary to ossification of interspinous and supraspinous ligaments on frontal radiographs
Tuberculosis:
- Paraspinal cold abscess (late feature)
- Abscess below T4 – typical fusiform shape (bird’s nest appearance); generalized broadening of mediastinum (too large abscess); globular shape (abscess under tension)
- Below the diaphragm – Along the course of psoas muscle
- Paring of healthy discs – “saw tooth” appearance
- Spine at risk sign for pediatric Pott’s spine: Lateral translation of vertebral column
Tumor pathology:
Metastatic lesions:
- Winking owl sign: Unilateral destruction of pedicle (may also be seen in primary lesions like aneurysmal bone cyst, osteoblastoma, etc.)
- Blind vertebra sign: Bilateral destruction of pedicle
- Nature of lesions: 30-50% destruction is needed before the lesions are visible on plain radiographs
- Osteolytic: Lung, thyroid, kidney, bladder, nasopharyngeal, colon, neuroblastoma
- Osteoblastic: Breast, prostate, lymphoma, carcinoid tumors, mucinous adenocarcinoma of GIT, pancreatic adenocarcinoma, bladder carcinoma, nasopharyngeal carcinoma, neuroblastoma, medulloblastoma
- Mixed
Primary lesions:
- Hemangioma: Jail bar or Corduroy cloth sign (vertical striated appearance due to replacement of normal cancellous bone by coarse, sclerotic trabeculae surrounded by fatty marrow or vascular spaces)
- Eosinophilic granuloma: Vertebra plana or Pancake or Silver dollar or Coin on edge vertebra (Decreased height of vertebra both anteriorly and posteriorly)
- Benign sclerotic tumors:
- Bone island (enostosis)
- Sclerosis secondary to osteoid osteoma
- Healed lesions such as cysts or fibroma
- Osteochondroma
- Malignant tumors:
- Chordoma (osteolytic pattern and soft tissue mass in sacrococcygeal region or vertebral body)
- Osteosarcoma (osteoid calcification of the tumour matrix, with marked mineralisation originating in the vertebral body that may manifest as an “ivory vertebra”)
- Bone lymphoma (Sclerotic vertebral body)
- Multiple myeloma or Solitary plasmacytoma:
- Lytic bone lesions
- Pathologic fractures
Abdominal Aortic Aneurysm: area of curvilinear calcification in the paravertebral region on either abdominal or lumbar spine radiographs
On Lateral View
Congenital pathology:
- Bar and block vertebra
Traumatic pathology:
- Decreased vertebral height
- Widened interspinous space
- Fracture dislocation (The anterior and posterior vertebral lines will demonstrate malalignment, with disruption of the facets posteriorly)
Osteoporotic vertebral fracture:
Loss of horizontal trabeculae that resists the axial load.
Genant’s classification:
- Wedge fracture
- Biconcave fracture (with endplate depression)
- Burst fracture
Sugita’s classification:
- Concave
- Dented
- Swelled-front
- Bow-shaped
- Projecting
Spondylolisthesis:
- Meyerding grading: Based on the position of the posterior margin of the upper vertebra over the upper end-plate of the inferior vertebra, which is divided into four equal parts from posterior to anterior.
- I – <25%
- II – 25 to 50%
- III – 50 to 75%
- IV – 75 to 100%
- V – Spondyloptosis (>100%)
- Retrolisthesis: Posterior shifting of cephalad vertebra over caudal vertebra
- Slip angle: Angle between the end plates of S1 and L5
- Dysplastic spondylolisthesis:
- Doming of sacrum
- Facet hypoplasia
- Vertical sacrum
Angle of kyphosis (K) in Pott’s spine:
- Dickson method: Angle between a line drawn from along the posterior margin of the bodies of the healthy vertebrae above and below the site of disease.
- Konstam’s method: Angle formed by the lines through the superior endplate of the normal vertebra proximal to the affected vertebrae and the inferior endplate of the normal vertebra distal to the affected vertebrae.
- Angular kyphosis:
- Knuckle: Wedging of 1 vertebra
- Gibbus: Wedging of 2-3 vertebrae
- Round kyphosis: Moderate wedging of large number of vertebrae
- Kumar’s classification of Pott’s spine:
- I (Pre-destructive) – Straightening of spine
- II (Early destructive) – Diminished disc space, Paradiscal erosion, K <10 degrees
- III (Mild kyphosis) – 2 to 3 vertebrae involvement; K 10-30 degrees
- IV (Moderate kyphosis) – >3 vertebrae involvement; K 30-60 degrees
- V (Severe kyphosis) – >3 vertebrae involvement; K >60 degrees
Scheuermann’s disease:
- Thoracic kyphotic angle greater than 45°
- Irregular endplates
- Schmorl nodes
- Narrowing of the intervertebral disc
- Vertebral wedging (local kyphosis >5º) must be present in at least one vertebral body, according to Sachs and Bradford’s criteria, or in three adjacent vertebral bodies, according to Sorensen’s criteria.
Ankylosing spondylitis:
- Syndesmophyte: vertical bone bridges
- Bamboo spine appearance: due to ossification of anterior and posterior longitudinal ligament
- Vertebral body squaring
- Romanus lesion/Shiny corner sign (florid anterior spondylitis; early feature): small erosions at the corners of vertebral bodies with reactive sclerosis
- Andersson lesion (florid discitis; late feature): irregularities and erosions of the vertebral endplates, not related to the anterior or posterior edge but rather to the central portions of the intervertebral discs
- Chalk stick/Carrot stick fractures
In psoriatic and reactive spondyloarthropathy, bone bridges tend to be coarser and more prominent.
Infectious pathology:
- Spondylodiscitis: Destruction of two adjacent vertebral endplates with narrowing or disappearance of the disc space (takes 2-8 weeks to appear), which may lead to acquired block vertebra
- Tuberculosis:
- Sites:
- Paradiscal
- Central
- Anterior
- Appendiceal (pedicles, laminae, spinous process or transverse process)
- Synovial
- Typical findings:
- Osteopenia
- Spondylodiscitis:
- Earliest: Osteopenia, Narrowing of disc space (due to destruction or prolapse)
- 1st trabecular destruction takes 3-5 months to appear
- Anterior vertebral collapse (knuckle, gibbus, rounded kyphosis)
- Concentric collapse like vertebra plana (in central type of TB)
- Atypical findings:
- Erosion or scalloping of the anterior vertebral wall without involvement of disc (due to subligamentous spread)
- Anterior subperiosteal lesion mostly where aorta is in close proximity permitting transmitted pulsations to the abscess (aneurysmal syndrome)
- Noncontiguous vertebral involvement
- Isolated involvement of neural arch
- Central bony lesions without disc involvement
- Ivory vertebra (disease focus surrounded by sclerotic vertebra)
- Tall vertebra (when disease occurs during the growth period, i.e. before the disappearance of growth zones)
- Signs of healing:
- Sharpening of irregular paradiscal margins
- Reappearance and mineralization of trabeculae
- Bony ankylosis (if disc is completely destroyed)
- Spine at risk signs for pediatric Pott’s spine:
- Facet joint separation at the apex of curve
- Posterior retropulsion at the apex of curve
- Toppling sign (line along the anterior surface of lower normal vertebra intersects above the middle of upper normal vertebra; normally intersects the inferior surface of upper normal vertebra)
- Lateral translation of vertebral column (seen in AP view)
- Sites:
Metabolic pathology:
- Paget’s disease (often in lumbar spine): Picture frame vertebra (Bone is expanded, cortex is thickened and trabeculae is coarse)
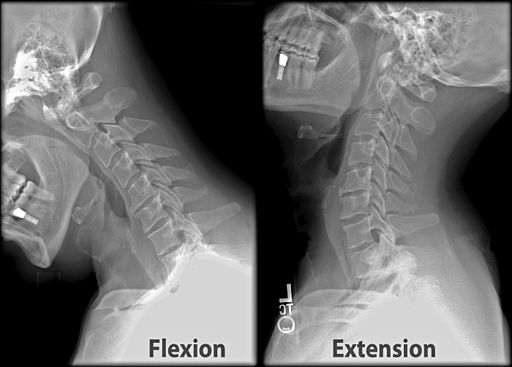
Dynamic lateral (flexion-extension) views
Spinal instability can be diagnosed with:
a. Sagittal plane translation/displacement:
- C-spine: >3.5 mm
- T-spine: >2.5 mm
- L-spine: >4.5 mm
b. Sagittal plane rotation:
- C-spine: >20 degrees
- L-spine:
- >15 degrees at L1-L2, L2-L3 and L3-L4
- >20 degrees at L4-L5
- >25 degrees at L5-S1
45 degrees Oblique View
In the oblique view an imaginary “Scotty dog” can be visualized with –
- Transverse process: nose
- Superior articular process: ear
- Inferior articular process: front legs
- Pars interarticularis: neck
Scotty dog with elongated neck or “collar”: Spondylolysis without slip
Decapitated scotty dog: Isthmic spondylolisthesis
Global analysis of Spine
Lateral view
Cobb angle: Choose the most tilted vertebrae above and below the apex of the curve. The angle between intersecting lines drawn perpendicular to the top of the top vertebrae and the bottom of the bottom vertebrae is the Cobb angle.
- Thoracic:
- Hypokyphosis: <20 degrees
- Kyphosis: 20-45 degrees
- Hyperkyphosis: >45 degrees
- Lumbar:
- Hypolordosis: <40 degrees
- Lordosis: 40-60 degrees
- Hyperlordosis: >60 degrees
- Sagittal alignment:
- Proximal thoracic kyphosis: between T2-T5
- Main Thoracic kyphosis: between T5-T12
- Thoracolumbar: T10-L2
- Lumbar: T12-S1
Sagittal balance:
- A plumb line is dropped from C7 center and another plumb line drawn from posterosuperior corner of S1
- Neutral balance: C7 plumb line passes within 5 cm of posterosuperior corner of S1
- Positive balance: C7 plumb line passes >5 cm anterior to posterosuperior corner of S1
- Negative balance: C7 plumb line passes >5 cm posterior to posterosuperior corner of S1
PELVIC MORPHOLOGY
Pelvic incidence: (PI) The angle created by a line drawn from the midpoint of the femoral heads to the midpoint of the superior endplate of S1 and a line drawn perpendicular to a line drawn parallel to the superior endplate of S1
- Normal: 40-65 degrees
- High pelvic incidence: Associated with spondylolisthesis and spondylolysis
Pelvic tilt (PT): The angle subtended by a vertical reference line (VRL) originating from the center of the femoral
head and a line from the center of the femoral head to the midpoint of the sacral end plate; it refers to compensatory efforts to maintain upright position
- Normal: 10-25 degrees
Sacral slope: (SS) The angle subtended by a horizontal reference line (HRL) and the sacral end-plate line; it sets the pitch of L5, thus dictating the lordotic movement
- Normal: 30-50 degrees
PI is measured from static anatomic structures. PT and SS on the other hand are position dependent because they are dependent on the angular position of the sacrum/pelvis in relation to the femoral heads that changes with standing, sitting, and lying down.
PI = PT + SS
Pelvic anteversion: High SS and Low PT
Pelvic retroversion: Low SS and High PT
T1 pelvic angle: Angle between a line drawn from the midpoint of the femoral heads to the midpoint of the superior endplate of S1 and a line drawn from the midpoint of the femoral heads to the center of the T1 vertebral body.
- Severe deformity: >20 degrees
- Goal of spondylolisthesis surgery: ~10 degrees
Ideally, a sagittal vertical axis (SVA)-posterosuperior S1 distance <40 mm, a PI-LL mismatch within 10º and a PT <20º have been considered the goals for appropriate sagittal alignment.
AP view
Cobb angle: Scoliosis – >10 degrees
- Curves according to location of apex:
- Main Thoracic (MT): T2 through T11-T12 disc
- Thoracolumbar (TL): T12 to L1
- Lumbar (L): L1-L2 disc through L4
- Structural curves:
- Major curve (always considered structural): largest curve (MT in Lenke 1-3; MT or TL/L in Lenke 4; TL/L in Lenke 5-6)
- Minor curves:
- Side-bending cobb angle ≥ 25°
- Regional kyphosis (T2-T5 for PT; T10-L2 for MT & TL/L) ≥ +20°
Coronal balance:
- C7 Plumb Line (C7PL): a line dropped parallel to the vertical edge of radiograph from middle of C7 vertebral body
- Central Sacral Vertical Line (CSVL): a line ascending parallel to the vertical edge of radiograph from midpoint to S1 endplate
- Coronal compensation: C7PL = CSVL
- Apical vertebral translation (AVT): measurement of perpendicular line from C7PL/CSVL to center of the apex vertebra
- Coronal decompensation: C7PL ≠ CSVL
- Apical vertebral translation (AVT):
- Measurement of perpendicular line from C7PL to center of the apex vertebra for PT and MT
- Measurement of perpendicular line from CSVL to center of the apex vertebra for TL and L
- Apical vertebral translation (AVT):
- Positive balance: the plumb line passes to the right of the midline, by >2 cm
- Neutral balance: the plumb line passes within 2 cm of the midline
- Negative balance: the plumb line passes to the left of the midline, by >2 cm
T1 tilt angle:
It is the angle formed by the intersection of a line drawn along the T1 cephalad endplate and a line parallel to the horizontal reference line.
- Negative: When the right edge of T1 vertebral body is up
- Positive: When the left edge of T1 vertebral body is up
Clavicular angle:
It is the angle formed by the intersection of a line touching the 2 highest points of the clavicle and a line parallel to the horizontal reference line.
- Negative: Angle subtended with right shoulder up (consistent with directionality of T1 tilt angle)
- Positive: Angle subtended with left shoulder up (consistent with directionality of T1 tilt angle)
Radiographic shoulder height (RSH):
It is the linear distance measured in millimeters between the superior horizontal reference line (SHRL), which passes through the intersection of the soft tissue shadow of the shoulder and a line drawn vertically up from the acromial clavicular joint of the cephalad shoulder, and the inferior horizontal reference line (IHRL) constructed in a similar fashion over the caudal acromial clavicular joint.
- Negative: Right up
- Positive: left up
Apex: The vertebra or disc with the greatest rotation or farthest deviation from the center of the vertebral column.
End vertebra (EV): Most tilted vertebra at cephalad and caudal end of the curve.
Neutral vertebra (NV): Most cephalad vertebra below the apex of the major curve whose pedicles are symmetrically located within the radiographic silhouette of the vertebral body.
Stable vertebra (SV): Most cephalad vertebra immediately below the end vertebra of the major curve that is most closely bisected by the CSVL.
Risser grade: Iliac crest and it’s apophysis ossifies from front to back –
- R0 – Ossification center not visible
- R1 – Up to 25% is ossified
- R2 – Up to 50% is ossified
- R3 – Up to 75% is ossified
- R4 – Up to the whole of the apophysis is ossified
- R5 – Fusion of ossified iliac apophysis to ilium
For skeletal maturity, open versus closed triradiate cartilage of the acetabulum can also be assessed.
Nash Moe Rotation or Apical Vertebral Rotation:
The half vertebra on the convex side of curvature is divided into three segments, and rotation is quantified on the basis of the pedicle location in regard to the segments:
- Grade 0 – Pedicles are symmetric
- Grade I – Pedicle slightly toward midline
- Grade II – Pedicle 2/3rd toward midline
- Grade III – Pedicle is in midline
- Grade IV – Pedicle beyond midline
Rib Vertebral Angle Difference (RVAD):
A line is drawn a perpendicular to the apical vertebral endplate. Another line is drawn from the mid-neck to the mid head of the corresponding rib. The angle formed by the intersection of these lines is the Rib Vertebral Angle or RVA. The difference between the values of the rib vertebral angles on the concave and convex sides of the curve is rib vertebral angle difference or RVAD.
- RVAD >20 degrees is considered as progressive
Thoracic truncal shift: Distance in mm between CSVL and VTRL (Vertical trunk reference line). VTRL is a plumb line dropped from midpoint of a horizontal reference line connecting center of apex vertebra/disc to the convexity of ribcage on both the sides.
- Positive: Trunk shift to right
- Negative: Trunk shift to left
Pelvic obliquity: Angle between a line connecting 2 tips of sacral ala or 2 most proximal points of iliac crest or sulcus of S1 on each side (all are Pelvic coronal reference line; PCRL) and Horizontal reference line (HRL).
Leg length discrepancy (LLD): Distance between the horizontal line tangent to the top of higher femoral head (Femoral Horizontal Reference Line or FRHL) and a similar line through the top of lower femoral head.
Approaching X-rays in Exams
A. Describe the X-ray: PA and lateral standing X-ray of lumbar/thoracic/cervical/full spine showing … (mention immature skeleton if you see a physis)
B. Lateral X-ray:
- Normal curves – cervical and lumbar lordosis, thoracic kyphosis.
- Abnormal curves – exaggerated thoracic kyphosis, loss of lumbar/cervical lordosis, cervical kyphosis.
- Disc height maintained or lost at any level. Fuzzy end plates could be a sign of discitis.
- Facet arthritis.
- Primary canal stenosis as evident by short pedicles.
- Fracture – compression, burst, stable or unstable fracture.
- Sagittal balance of full spine weight-bearing lateral – normal, positive or negative.
- Spondylolisthesis – is it isthmic (if lysis of pedicles seen) or degenerative (facet arthropathy)?
• Meyerding grading
• Pelvic tilt, sacral slope and pelvic incidence.
C. AP X-ray:
- Cancer – winking owl sign – destruction of pedicle due to cancer.
- Degenerative – facet arthritis or scoliosis (curve can be in either direction).
- Idiopathic scoliosis – usually right convex in the thoracic spine (away from the heart); rissers grade to check for progression
- Prolapsed disc – list away from nerve compression.
- Evaluate pedicles always on AP view. Absent pedicle may be seen in metastases, aneurysmal bone cyst, osteoblastoma, trauma or congenital absence of pedicle.
The texts are not very useful without the appropriate images. Please refer to the links below for the images and further description of the parameters.
Sources and Further Reading:
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7596402/
- https://www.oref.org/docs/default-source/default-document-library/sdsg-radiographic-measuremnt-manual.pdf
- https://surgeryreference.aofoundation.org/spine/deformities/spondylolisthesis/further-reading/clinical-evaluation
- https://pubs.rsna.org/doi/10.1148/radiol.2015142404
- https://sajr.org.za/index.php/sajr/article/view/294/384
- https://www.imageinterpretation.co.uk/thoracolumbar.php
- Karpe, P. (2019). Spine. Postgraduate Orthopaedics, 121–157. doi:10.1017/9781108686624.007
- Karpe, P. (n.d.). Spine clinical cases. Postgraduate Orthopaedics, 88–112. doi:10.1017/9781316091685.013

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.

thanks for making my life easy
Nice information