Anterior Cruciate Ligament (ACL)
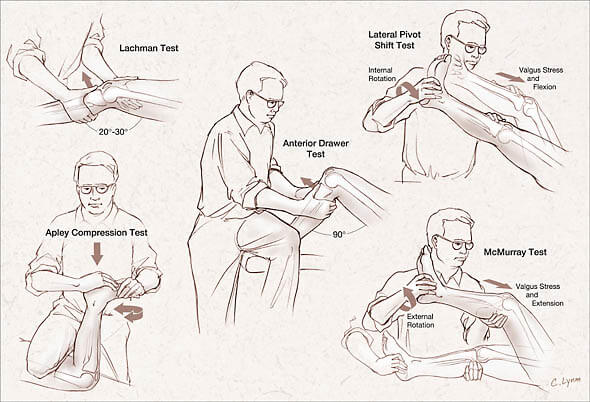
Lacchman’s test
It is performed with the patient supine and the knee flexed 20–30°. The examiner grasps the distal femur (from lateral side) with one hand and the proximal tibia with the other hand (from medial side). The lower leg is given a brisk forward tug in an attempt to identify a discrete endpoint. A positive test (indicative of injury) occurs when no endpoint is appreciated or there is increased anterior translation of the tibia relative to the unaffected side.
Anterior Drawer test
It is performed with the patient supine and the knee flexed to 90°. Both hands are placed around the proximal tibia with the thumbs approximated at the anterior tibial plateaus. The examiner quickly pulls anteriorly, without rotation, and feels for a discrete endpoint. The test is positive if no discrete endpoint is reached, especially compared to the unaffected side.
The Lachman test is the test of choice for the acutely injured knee. The reasons for this are:
- An acute injury with an associated haemarthrosis prevents knee flexion to 90 degrees
- Protective spasm of the hamstring muscles is negated with the joint extended.
- With the knee tested in extension, the acutely convex configuration of the posterior surface of the medial femoral condyle is disengaged from the “door-stop” effect of the posterior hom of the medial meniscus. The relatively flat configuration of the anterior aspect of the femoral condyle doesnot obstruct anterior translation of the tibia.
Pivot Shift test
Assesses: MCL + ACL (Rotator Instability)
The test is performed with the patient in a relaxed, supine position. The knee to be tested should be fully extended and the hip flexed to approximately 30 degrees. One of the examiners hands holds heel of the foot of the leg to be tested. The examiner’s other hand is on the lateral aspect of the proximal tibia, with the fifth metacarpal near the head of the fibula.
From the starting position the examiner holds the lower leg in internal rotation and slowly flexes the knee while putting a moderate valgus and internal rotation force on the proximal tibia.
This test is considered positive if the proximal tibia subluxes anteriorly on the distal femur at about 30 degrees of flexion. In a positive test, the proximal tibia will clunk back into place while returning the knee to extension. Flexion past approximately 40 degrees will also reduce the tibia due to the iliotibial band.
Posterior Cruciate Ligament (PCL)
Posterior Drawer Test
This test is performed with the patient supine and the knee flexed to 90°. There are two different ways it may be performed. The first is the opposite of the anterior drawer test. Absence of a discrete endpoint with posterior force applied to the tibia is considered positive. The second approach is positive if anterior force applied to the tibia corrects a posterior subluxation or “sag” of the affected knee.
Reverse pivot shift test
Performance of this test is with the knee flexed to approximately 80°-90°, with a valgus and external rotation force applied to the knee. In this position, the tibia would be subluxed posterolaterally for a positive test. The knee is then extended. If the tibia is posterolaterally subluxed, the iliotibial band will reduce it as it goes from a flexor to extender of the knee and a visible reduction of the tibia on the femur can occur.
Menisci
McMurray Test
The McMurray test is performed with the patient supine and the examiner grasping the medial aspect of the affected knee with one hand and the patient’s heel with the other hand. A valgus force is generated and the tibia internally rotated as the knee is moved from a fully flexed position to full extension. The test is repeated while externally rotating the tibia. Any “popping” or pain along the joint line is considered a positive test.
Apley’s Compression or Grind Test
It is performed with the patient prone and the knee flexed to 90°. A downward force is generated along the long axis of the tibia while simultaneously externally rotating it. If pain is increased, the test is positive.
Thessaly Test
The test is performed with the patient in standing with full weight bearing on the side to be tested. The foot should be flat on the floor. The non-test leg is flexed at the knee to prevent the foot on the non-test leg from contacting with the ground.
The examiner supports the patient by the outstretched hand or hands to provide balance. The patient flexes the knee to be tested to approximately 20 degrees (an additional test at 5 degrees is sometimes carried out). While in this flexed position, the patient rotates the femur on the tibia three times, both internally and externally.
A positive test is indicated by reports of pain on the joint line or by joint locking or catching.
Collateral Ligaments
Valgus stress test for Medial Collateral Ligament
It is performed with the patient supine and the knee in 20° of flexion. With one hand on the lateral aspect of the knee and the other on the foot, the examiner gently abducts and externally rotates the lower leg. Increased laxity compared to the unaffected side is considered a positive test for medial collateral ligament (MCL) injury.
Varus stress test for Lateral Collateral Ligament
In the varus stress test, the examiner adducts and internally rotates the lower leg to assess the stability of the lateral collateral ligament (LCL).
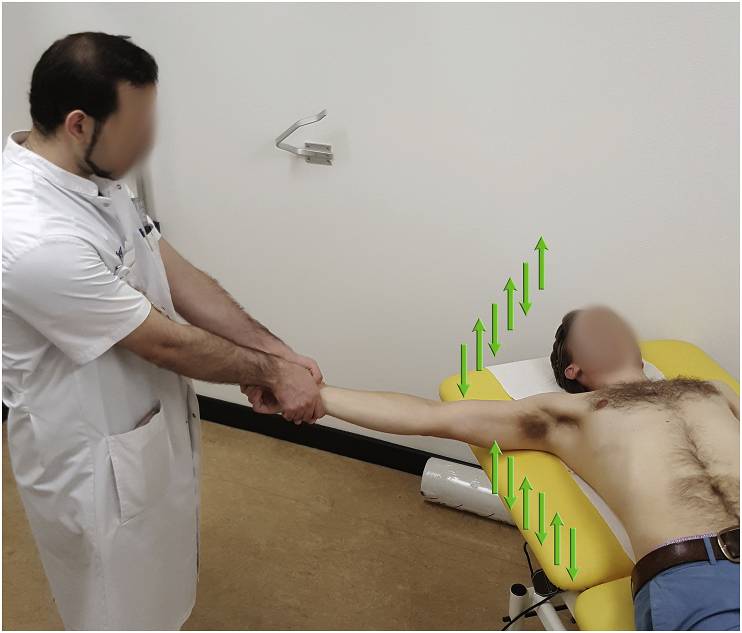
Apley’s Distraction Test
Patient prone with knee flexed 90°
Examiner stabilizes patient’s thigh by placing knee over the patient’s distal posterior thigh
Examiner then applies long axis distraction above the maleoli at the ankle (pulls up) and internally and externally rotates leg.
Pain with distraction: Capsule/ligamentous lesion at the knee or collateral ligament sprain.
Decreased pain following distraction: Meniscal lesion.
Very good explanation to the anteromedial instability of the knee.