As a Doc. whenever you treat a patient, the success of treatment depends upon whether you come up with the right diagnosis or at least a right set of differential diagnoses.
To achieve the above mention goal the KEY is EFFECTIVE COMMUNICATION.
And I can talk to you for an hour without actually extracting anything from that conversation that’s going to help me to reach my goal.
So make your conversation effective by knowing the Objectives of your conversation.
- To Gain the trust of historians so that you can extract information from patients or attendants (as in case of pediatric, mentally unstable, or an unconscious patient).
- To make sure historian is a reliable source of information and knows about patient and his condition(in case of history is being taken from attendant)
- To know what is relevant information which is going to help me to achieve my goal.
- To extract an ample amount of relevant information.
- To discuss in depth; To have enough discussion with historians about what’s going on? That you don’t get fooled by superficial information or misinterpret the information.
Don’t forget to add “ICE” to your history to incorporate patient’s perspective.
History taking is one art and the other is History Presentation.
Keep in mind:
1. Your goal (to reach a diagnosis/differential diagnosis)
2. Key to achieve the goal i.e. effective communication
3. Objectives of your conversation
4. Presentation of the history

Let’s begin…
NOTE
Use these mnemonics so you can easily keep all points in your mind.
An example will be added for history presentation skills.
Approaching the patient
Mnemonic: R GIC
- R – Approach patient from the right side.
- G – Greet patient
- I – Introduce yourself.
- C – Take consent
Biodata of Patient (Personal details)
Mnemonic: No Available SOMA(neuronal cell body) so go for MultiDrug Therapy.
- N – Name
- A – Age
- S – Sex
- O – Occupation
- M – Marital status
- A – Address
- M – Mode of admission (OPD or Emergence)
- D – Date of admission
- T – Time of admission
Presenting Complaints (Chief complaints)
What is the disturbing problem that brings you to the hospital?
From how long you have this problem i.e. duration?
NOTE
- In case more than 1 presenting complaint write in chronological order i.e. one with longer duration should be written first.
- Complains should be less than 3-4 in number.
- Write in patient words doesn’t add to it.
- Write symptom(s) and not the diagnosis.
- You can use a good medical term that describes the symptom like “hematemesis” for blood in vomitus.
- Don’t make a sentence out of complaint e.g. write abdominal pain not pain in the abdomen
- Make your differentials of presenting complain and in history of presenting illness rule in & rule out to narrow down as much as you can.
History of Presenting Illness (HOPI)
Symptom analysis: Get to know the symptom in a way it leads us towards a diagnosis. e.g. abdominal pain doesn’t help me to establish the diagnosis but knowing more about the characteristic of a symptom does.
So following are the characteristics you should know about the symptom for analysis.
General characteristics for all symptoms:
Mnemonic: O D PARA
O – Onset of symptom sudden/Gradual
D – Duration of symptoms
P – Progression (is the symptom progressively worsening or it’s static)
A – Aggravating factors
R – Relieving factors
A – Association (to know the other symptoms accompanying the main symptom which help us to rule in or rule out a differential diagnosis)
Additional Characteristics that you should know for symptoms that are fluid in nature (blood/bleeding, vomiting, loose motion)
Mnemonic: FVC3
F – Frequency/# of episodes
V – Volume/amount
C – Color
C – Content
C – Consistency
Additional Characteristics For pain
Mnemonic: Royal Challengers Team Smashes 3 goals (RCTS3)
R – Radiation
T – Timing
C – Character
S – Site of pain
S – Severity of pain
S – Shifting of pain
Risk factor assessment: To get a clue about what makes a patient susceptible to get this disease, e.g. history of surgery/ dental procedure and its association with hepatitis B/C
Associations
- The purpose is to rule in a differential or rule it out.
- Ask for other symptoms that patient have.
- This helps you to decide that the set of symptoms that patient have, fits best in a particular diagnosis.
- It helps you to know which system is involved in the disease process.
Systematic Review
Quickly ask about the cardinal symptoms of diseases of each system.
This section is important to know about the baseline health status of the patient. Patients may ignore less bothering symptoms due to the severity of current symptoms. To make sure no aspect of the illness is missed quickly enquire the patient for the following symptoms.
- General – Sleep pattern, appetite, weight gain, or loss.
- Cardiovascular System – Breathlessness, palpitation, orthopnea, chest pain, bilateral pedal edema.
- Respiratory System – Dry/Productive cough, hemoptysis, dyspnea, wheezing.
- Alimentary System – Nausea, vomiting, abdominal pain, dyspepsia, dysphagia, diarrhea, constipation, haematemesis, melena, jaundice, abdominal distention.
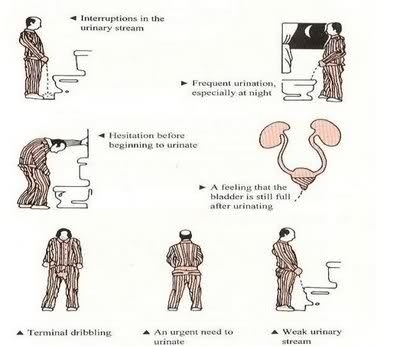
- Urinary System – Flank pain, hematuria, burning micturition, nocturia, the passage of gravel in the urine, any foul smelly discharge.
- Nervous System – Weakness, numbness, tingling, headache, dizziness, fits, visual disturbance.
- Skin – Rash, itch, colored spots.
- Locomotor System – Joint pain, stiffness, swelling, restriction of joint movements.
- Endocrine – Polyphagia, polyuria, polydipsia, heat or cold intolerance, weight gain or loss, menstrual irregularities
- ENT – Earache, discharge, lesion, dizziness
- Eye – Headache, orbital pain or swelling, loss of visual field, any sight-related issue.
History of any comorbidities
- Any known illness
- Duration of disease
- Any complication regarding disease
- The type of treatment and how long he has been taking this treatment (if taking any)
- Is he compliant to treatment?
- Is there any history of diabetes, hypertension, ischemic heart disease, asthma, hepatitis B/C?
Remaining History Points
Mnemonic: MAFOSTA PS DMI
MAFOSTA is an acronym that sounds like Ma- fos- ta.
So, MAFOSTA PS DMI covers all other points of history taking i-e;
M – Previous MEDICAL Record (Past Medical and Past surgical History)
- Any history of previous illness, the type of treatment taken and did he recover or not
- Self-medication or Quack medication
- Any previous surgery, why & when
A – history of Allergies
- Any known allergy to food, drug, pollen/dust.
- How your allergy manifest itself (sneezing/urticaria)
- Any atopic disorder e.g asthma.
F – Family History
- Any comorbidity running in family-like diabetes, hypertension, ischemic heart disease, malignancy, congenital abnormalities
- Any history of contagious disease in the family members.
O – Occupational History
- Type of Job
- How long you have been doing this
- Any previous job and its duration
- Any chemical, patient is aware of being exposed to at the present or previous workplace
- Is any safety precaution taken
- This is very important in Respiratory tract systems such as pneumoconiosis.
S – Sexual History
- Any symptom regarding genital tract
- Any lesion in genitalia
- Any previous screening for STDs
- Any history of infected with STDs
- Sexual Partner/partners & any information about their STDs status.
T – Travel History
Any history of a recent visit made in any particular area especially important when you are suspecting a disease prevalent in that part of the world.
A – Any other
- Any Significant thing patient wants you to know.
- Ask this as an open-ended question at the end of history taking.
- Is there anything that you want to share with me?
P – Personal history
- Dietary habits
- Sleep pattern
- Bowel & Bladder habits
- Smoking(active/passive)
- Previously smoker (left how long ago?)
- Exercise routine
S – Social history
- Source of income
- Family members
- Income per capita
- Residency (own/rent)
D – Drug abuse History
- Any history of being a drug abuser
- Admitting in Rehabilitation center
- Was rehabilitation successful or not
- Drug overdose for which he needed any emergence treatment or on & off the use of any recreational drug
M – Menstrual/Gynecological History & Mental health
Gynecological history
- Length of the menstrual cycle
- Regular/Irregular
- Any compliant of dysmenorrhea
- Any known gynecological ailment
- In married females Parity, any history of Abortion, mode of delivery/ies, history regarding the use of contraception, any gestational comorbidity.
Mental health
- Interaction with family, friends and colleagues’
- Personality type (introvert/extrovert)
- Being ever bullied for
- Any known psychotic illness
- Any history for any violence committed
- Any history of being in police custody
- Any history of depression or consulting a psychiatrist
I – Immunization History
- What are the Diseases against which the patient has been vaccinated?
- How long?
- Any booster shot(s)
I – Investigations
That has been previously done either for this disease or any other.
It’s necessary to have a quick look at previous investigations because it may give you a piece of information that the patient is missing maybe deliberately or due to a lack of awareness.
NOTE:
Be careful while taking history because someone has to share their private and sensitive information with you so don’t laugh or give any disturbing facial expression.
Respect their sentiments.
Don’t be judgmental about the patient, his morals, or social status.
He is just a patient and you have to heal his damage that’s your job.
Presentation
My patient, a school teacher, Mrs. Ashley James 40 years old resident of the west street, California presented through emergence department on april/5/2009 at 4 pm with the complaint of:
- Abdominal pain X 8 hours
- Vomiting X 5 hours
History Of Present Illness:
My patient is normoglycemic, a known case of asymptomatic gallstones for 4 years and hypertension for 3 years for which she is taking oral Amlodipine 5mg OD daily for the last 2 years, has good compliance to the treatment and her hypertension is controlled with the current regimen. She was in the usual state of health 8 hours back when she developed sudden, very severe, sharp and progressive epigastric pain for 8 hours radiating to her back which was relieved by leaning forward, aggravated by taking meal & was associated with 5 episodes of nonprojectile vomiting with copious yellow-green watery vomitus; containing food particles of the meal taken 12 hours back. The pain is not associated with headache, fever, neck stiffness, sweating, burning micturition, radiation to arm, neck or groin, abdominal distension and obstipation or junk food intake.
She is a known case of gallstones for the last four years which is an incidental finding on her abdominal ultrasonography. She never drinks alcohol.
Her sleep and appetite are good. There is a history of exertional dyspnea. There is no history of chest pain, cough, hemoptysis, wheezing, headache, fits, motor weakness, polyphagia, polydipsia, polyuria, weight gain or loss, melena, jaundice, urinary complaints and rash.
Past medical history:
She has no history of such episode previously.
10 years back she was diagnosed with iron deficiency anemia during her antenatal visits for which she was advised to take oral iron supplements for a period of 1 year. According to the patient, her current hemoglobin is 13g/dl.
Past surgical history:
She had 1 cesarean section, 10 years back due to the transverse lie of the baby. The wound healed without any complication.
Allergies:
She is allergic to the dust. Whenever exposed to the dust, she had multiple bouts of severe sneezing which was relieved by taking oral antihistaminics.
Family history:
There is no family history of such illness. There is no history of ischemic heart disease, hypertension, diabetes, asthma, and hepatitis B/C in any of her family members.
Occupational history:
She is a school teacher for the last 15 years.
Sexual history:
She is happily married to Mr. James smith for 14 years. She has no complaint of any genital tract symptom or lesion. She and her partner never had any screening for STDS.
Travel history: Not significant
Personal history:
She is non-smoker, sleeps comfortably for 8 hours every day, has normal bowel and bladder habits and she goes to gym every day for an hour.
Social history:
She lives in her own house with her 9-year-old kid. She doesn’t have history of any Drug abuse.
Gynecological history:
She has a regular menstrual cycle of 4/35 associated with severe dysmenorrhea. She is using injectable contraception for the last 8 years.
Investigations:
Her 4-year-old ultrasonography report shows a single gallstone of 3 cm
Any other:
She was transfused a pint of packed cells during her c/sec. 10 years back.
She is a compassionate individual with excellent presentation, research, and communication skills. Organized and driven with an impressive list of achievements and excelling within high-pressure environments, she is skilled at applying various learning methods and tools to make study easy. She is interested in reading and writing medicine-related articles.
Very nice and elaborate explanation. I would like to add few things:
1. Socioeconomic status can be assessed using Kuppu-swamy index
2. Smoking must be quantified in smoke-years
3. Alcohol intake must be quantified in Units
4. Family history may require pedigree chart
5. Developmental history and Dietary history is necessary in pediatric patients
6. A 24 hour dietary recall can be used to assess dietary history
very informative and elaborate