Introduction
- Extracranial scalp AVMs are rare high-flow vascular shunts.
- Can cause massive blood loss & high-output cardiac stress.
- Steal phenomenon reversal: Sudden AV shunt removal → ↑SVR & ↓venous return → ↓BP
Case Description
- 10-year-old female
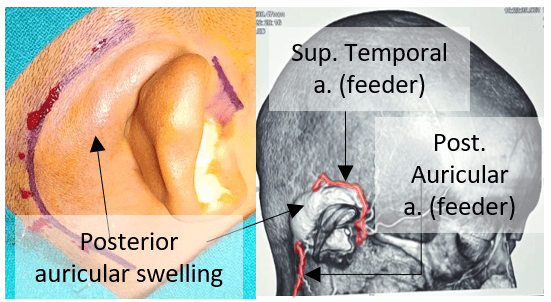
- Progressive right post-auricular swelling for 2 years (Fig. 1)
- Palpable thrill & audible bruit
- PAC: METS >4 & Stable vitals; Investigations – unremarkable (Echocardiography revealed EF 61%)
Anesthetic Challenges
| Airway & positioning | Hemodynamic instability |
| Massive blood loss | Hypothermia and metabolic disturbances |
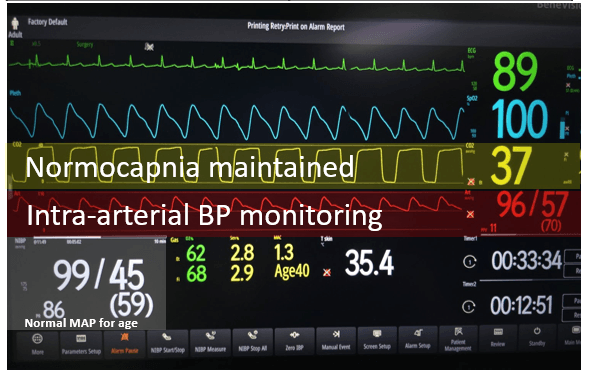
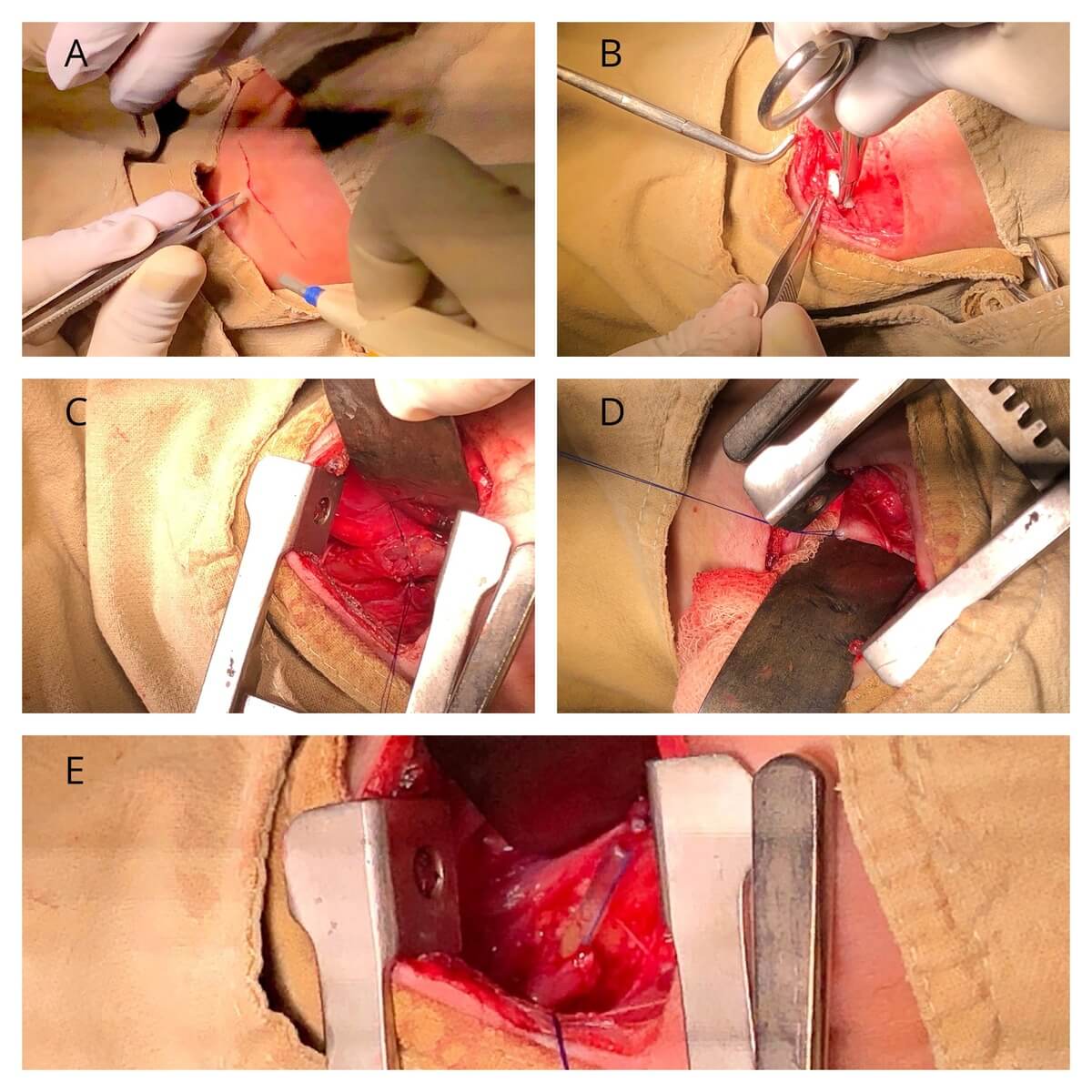
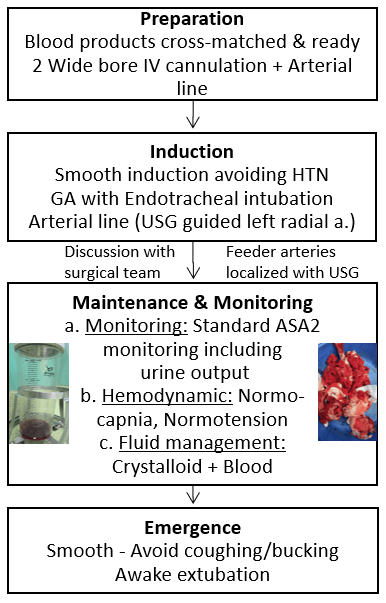
Intraoperative Management
Postoperative Considerations
- Ongoing bleeding & hemodynamic instability
- Delayed cardiac effects
- Adequate analgesia
| Pearls | Pitfalls |
| Anticipate hemodynamic shift after ligation | Under-estimated blood loss |
| Controlled hypotension during dissection | Venous air embolism (open scalp veins) |
| Normothermia +/- Tranexamic acid | Aggressive hypotension |
Conclusion
- Pediatric Scalp AVMs behave like systemic AV shunts.
- Anesthetic success depends on anticipation, monitoring & blood readiness.
Abbreviations:
- AVM: Arteriovenous Malformation
- HTN: Hypertension
- MAC: Minimum Alveolar Concentration
- TIVA: Total Intravenous Anesthesia
- GA: General Anesthesia
- SVR: Systemic Vascular Resistance
Reference: Shamim et.al. 2012 (JOACP)

Anesthesiology Resident (PGY-1) at Tribhuvan University Teaching Hospital, Institute of Medicine (TUTH, IOM). Her academic interests include perioperative medicine, regional anesthesia, and evidence-based practices in anesthesiology. She contributes scholarly articles on anesthesia to Epomedicine.