Case summary
A female neonate was born via emergency cesarean section at 36 weeks of gestation. The indication of LSCS was polyhydramnios with fetal bradycardia. The birth weight of the neonate was 1700 grams following which the baby was shifted to NICU for observation. I, as a surgical resident was called to NICU when the baby was just 16 hours of life. The cause of consultation was inability of the pediatric resident to pass the orogastric tube.
On examination:
- The baby was afebrile with maintained blood pressure and oxygen saturation in room air.
- Abdomen was soft, non-distended with no bowel sounds
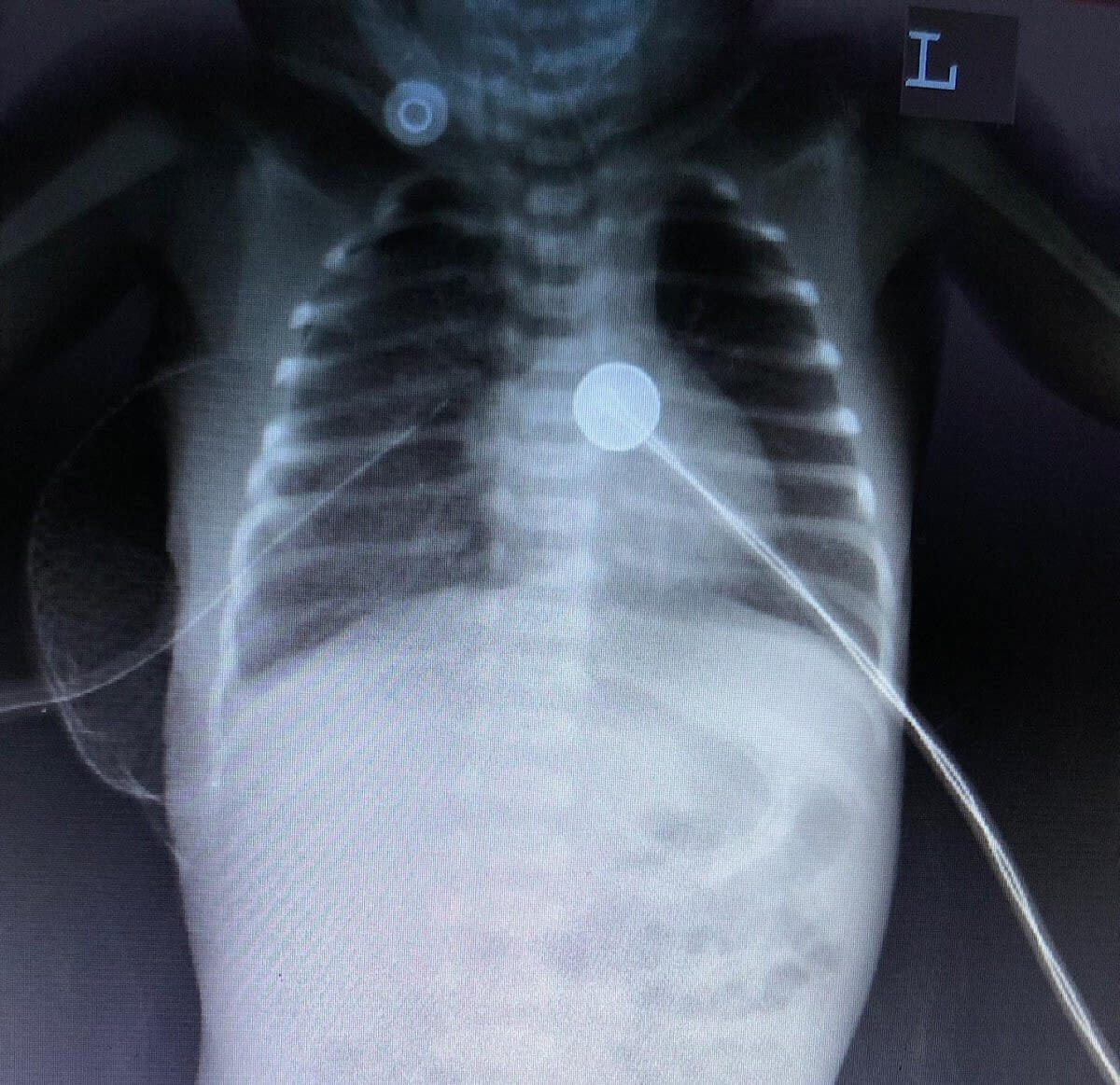
- Orogastric tube insertion attempted failed following which an urgent chest radiograph was ordered which revealed following findings:

This picture shows no gas shadows in abdomen indicating that the air has not passed into the GI tract even after 16 hours of life.
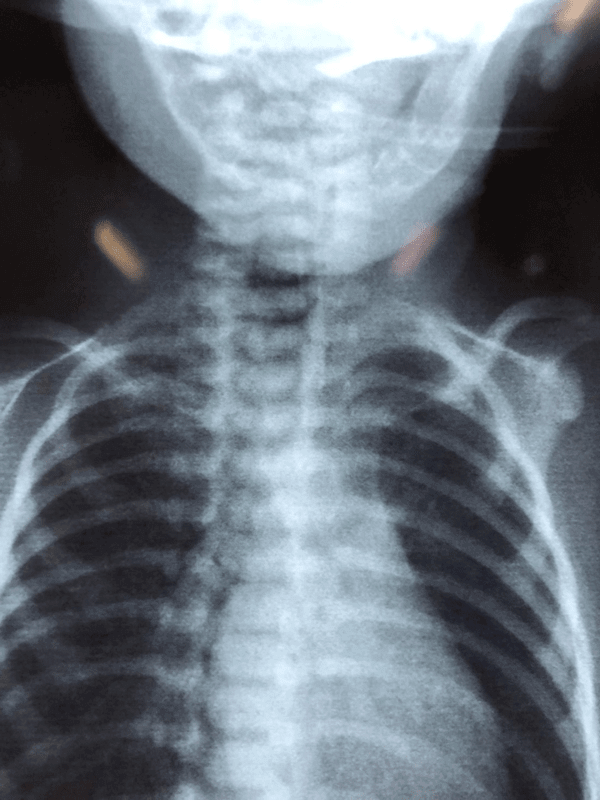
This is the chest radiograph taken after inserting feeding tube. This radiograph shows the coiling of feeding tube.
We drew following inferences from these 2 radiographs:
- Since there is no gas in the abdomen it points that there is discontinuity in the esophagus indicative of esophageal atresia.
- The coiling of the tube confirms the above inference.
- There is no fistulous connection between trachea and esophagus as there is no gas in the abdomen (if there was fistula the abdomen would have gaseous distention due to passage of air from the trachea into the GI tract).
We made a diagnosis of Gross type A esophageal atresia without fistula and planned for thoracotomy and proceed.
USG (abdomen) and echocardiography to rule out VACTERL association which were normal.
We shifted the patient in the operation theatre, general anesthesia was given following which right lateral thoracotomy was done and following findings were revealed.
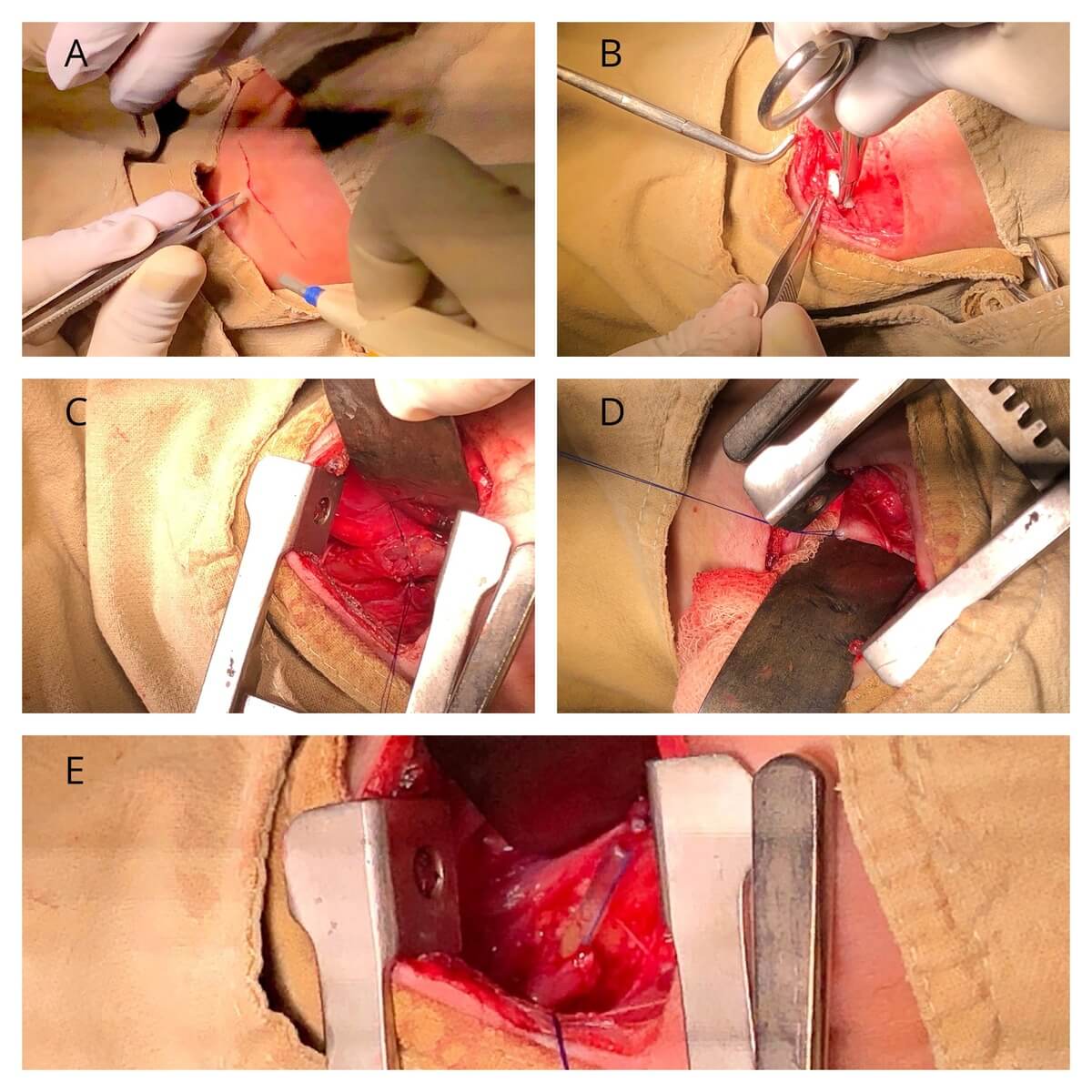
B – Incision was then opened in layers;
C – After exploration, the distal stump of esophagus identified;
D – Proximal stump was identified, opened and feeding tube is introduced;
E – The tube was then negotiated into the distal stump followed by primary end to end anastomosis (first posterior layer followed by anterior layer)
The distance between the 2 stumps was approximately 2.5 cm.
The incision was then closed in layers after placing mediastinal drain in situ.
Post operatively the baby was shifted to NICU for observation and further complication management.
Today is the 7th post operative day. Baby is feeding well and the abdomen has gaseous distension. Barium swallow revealed no leak. Hopefully the baby will recover well with no major complication noted as of now.
Discussion
Epidemiology:
- Birth incidence: 1 in 2500-3000 live births
- Male: female: 1.26:1
- No evidence of link between EA/TEF and maternal age when chromosomal cases are excluded.
- Risk of EA/TEF in second child among parents of one affected child: 0.5-2%
- This risk increases to 20% when more than one child is affected.
- Empirical risk of an affected child born to an affected person: 3-4%
- Relative risk in twins: 2.56
Risk factors:
- Use of methimazole in early pregnancy
- Prolonged use of OCPs
- Maternal diabetes
- Thalidomide uses in pregnancy
- Fetal alcohol syndrome
- Maternal phenylketonuria
Relevant embryology:
During 4th week of gestation foregut starts to differentiate into:
- Ventral respiratory part
- Dorsal esophageal part
Both of these are separated by formation of lateral tracheoesophageal fold which fuse in midline to form tracheoesophageal septum.
By 6-7 weeks the separation is complete.
Incomplete fusion results in defective formation of septum and results in abnormal communication between esophagus and trachea.
Associated anomalies with TEF/EA:
- Cardiac (13-34%)
- Vertebral (6-21%)
- Limb (5-19%)
- Anorectal (10-16%)
- Renal (5-14%)
Classification:
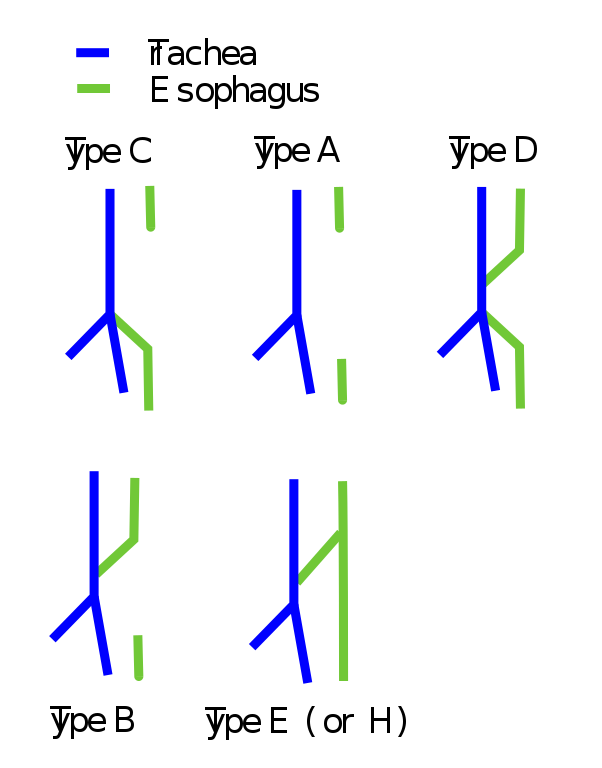
| Gross type | Description | Incidence | Remarks |
| A | Pure atresia without TEF | 7% | Proximal ends at azygous vein levelDue to increase distance anastomosis usually not possible |
| B | EA with proximal fistula | 2% | Fistula usually located at thoracic aperture or higher in neck |
| C | EA with distal fistula | 85% | Proximal- T2-T4 levelDistal- at carina or 1-2 cm higher |
| D | EA with proximal and distal fistula | <1% | – |
| E | H type fistula without EA | 4% | Usually, a part of VACTERL |
Diagnosis:
Antenatal:
- USG- mainstay of imaging
- Non-specific findings: polyhydramnios and absent/small stomach bubbles
- Combination of small stomach with dilated cervical esophagus (“the pouch sign”) is diagnostic
- USG sensitivity- 60-100%
Post-natal:
Presentation:
- Drooling of saliva
- Inability to drink milk
- Respiratory distress
- Mother with polyhydramnios
Catheter test:
10 Fr catheter is passed either through nose or mouth and a chest radiograph is obtained. This is illustrated in our case as well.
USG and echocardiography are done to rule out VACTERL association.
Treatment:
Treatment is surgical. The type of surgery depends on the type of EA/TEF.
In cases of pure atresia primary tension free end to end anastomosis is attempted whenever possible. If this is not possible then the options include feeding gastrostomy for maintaining nutrition of the baby and delayed anastomosis. If delayed anastomosis is not possible then esophageal replacement is considered.
If there is TEF then option is ligation of fistulous tract and primary repair of trachea and esophagus.
The approach of surgery (cervical or thoracotomy) depends on the level of EA or TEF. Generally, as a rule if it is present at or below T2 level thoracic approach is done and above it cervical approach is considered (this is not always true).

He is an avid reader, guitar player, melodious singer and old songs lover. He has a passion for making medical knowledge accessible and comprehensive.