Located in the middle cranial fossa on the side of the body of sphenoid bone
Size: 2 cm long and 1 cm wide
Walls:
Floor and Medial wall: Endosteal (Periosteal) layer of dura
Roof and Lateral wall: Meningeal (Fibrous) layer of dura
Extent:
Anteriorly: Upto the medial end of Superior Orbital Fissure (SOF)
Posteriorly: Upto the apex of petrous temporal bone
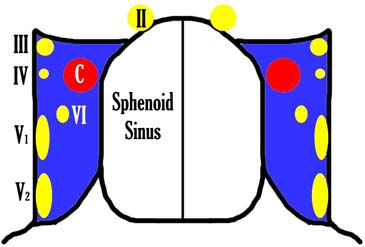
Contents of Cavernous sinus
These are closely related to the floor of sinus and are separated from the interior of sinus by endothelium.
Internal carotid artery (ICA) surrounded by sympathetic plexus (ICA comes out of the sinus by piercing the roof)
Abducent nerve (CN VI) – infero-lateral to ICA
4 nerves in the lateral wall:
Occulomotor nerve (CN III)
Trochlear nerve (CN IV)
Ophthalmic division of Trigeminal nerve (CN V1)
Maxillary division of Trigeminal nerve (CN V2)
Note: Mandibular branch of trigeminal nerve (CN V3) anatomically lies posterolateral to the cavernous sinus inferior to the trigeminal or gasserian ganglion.
Cavernous sinus coronal view – Arogersmd at English Wikibooks, CC BY-SA 2.5, via Wikimedia Commons
Relation to surrounding structures:
Medial: Pituitary fossa, Sphenoid sinus
Lateral: Temporal lobe
Mnemonic for structures inside and beside cavernous sinus: O TOM CAT (Occulomotor nerve, Trochlear nerve, Ophthalmic branch of Trigeminal nerve, Maxiallary branch of Trigeminal nerve, Carotid artery, Abducens nerve)
O O (III)
T A C C A T (IV)
O O (V1)
M M (V2)
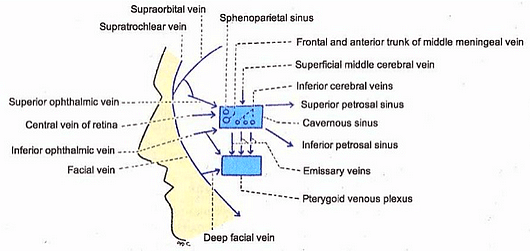
Tributaries (Incoming channels)
1. From orbit:
Superior ophthalmic vein
Inferior ophthalmic vein
Central vein of retina
2. From brain:
Superficial middle cerebral vein
Inferior cerebral veins
3. From meninges:
Spheno-parietal sinus
Middle meningeal sinus (vein)
Tributaries and Communications of Cavernous sinus
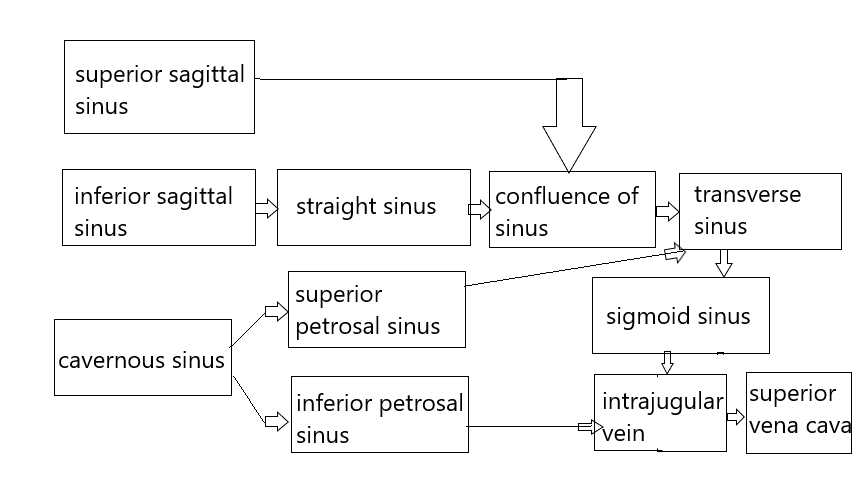
Communications (Draining channels)
Transverse sinus: via superior petrosal sinus
Internal jugular vein (IJV): via inferior petrosal sinus
Pterygoid venous plexus: via emissary veins (passing through foramen ovale, spinosum and lacerum)
Facial vein: via superior ophthalmic vein
Opposite cavernous sinus: via anterior and posterior inter-cavernous sinus
Note: In all communications, blood can flow in either directions.
Factors responsible for drainage of blood from cavernous sinus:
Expansile pulsation of Internal carotid artery (ICA) within the sinuses
Gravity
Position of head
Special features of Cavernous sinus
Lies between the 2 layers of dura mater
No muscle tissue in the wall
No valve, hence blood can flow in both directions
Cavernous/plexiform pattern interiorly
Internally lined by endothelium, which is continuous with the veins
Applied anatomy of Cavernous sinus
1. Cavernous Sinus Thrombosis (CST): Cavernous sinus can get infected from different septic foci as illustrated below:
2. Danger area/triangle/zone of face: The three points of triangle are the 2 corners of mouth and the bridge of nose. Infections from the face can spread in retrograde direction and cause thrombosis of the cavernous sinus via facial vein and pterygoid plexus.
3. Cavernous sinus syndrome: It is caused by various parasellar pathological condition that involves cavernous sinuses along with cranial nerves (3,4,5,6), Internal carotid artery and sympathetic plexus due to its close anatomical association and gives rise to various signs and symptoms in different combinations in different diseases.
4. Tolosa-Hunt syndrome: It is a painful ophthalmoplegia caused by nonspecific inflammation (noncaseating granulomatous or non-granulomatous) of the cavernous sinus or superior orbital fissure.
5. Carotid-cavernous fistula: It is an abnormal communication (direct or indirect) between cavernous sinuses and carotid artery or its branches.
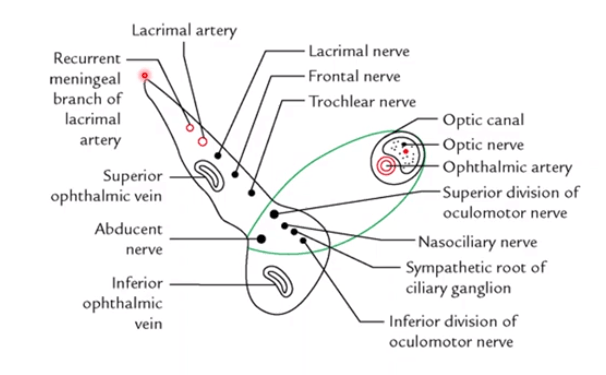
Superior Orbital Fissure (SOF) is a cleft between greater and lesser wing of sphenoid which connects orbit and middle cranial fossa. It is divided into 3 compartments by the tendinous ring (annulus of Zinn). Superior orbital fissure alone (Lateral compartment): Mnemonic: LFTS Superior orbital fissure in tendinous ring (Intermediate compartment):…
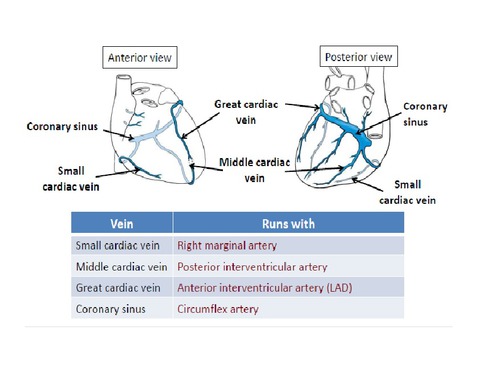
Mnemonic: CAT 1. Coronary sinus (50%): Drains blood from left side of heart → Thebesian valve → Right Atrium 2. Anterior cardiac veins (20%): Drain blood from right side of heart → Right Atrium 3. Thebesian veins/Venae cordis minimi (30%): Drain deoxygenated blood from endocardium and myocardium → Respective chamber…
Eye drops, nasal sprays, antihistamines, carrying your EpiPen wherever you go, avoiding certain environments like the plague, avoiding beloved pets or meticulously scanning ingredient lists for just about every food product you consume. All this and more are just another part of everyday life for people with allergies. Allergies might…

Please send me a copy.
Thanks.
Nice presentation
very nicely expressed
Great way of explanation