Surgical Principles
- Anterior dislocation of femoral head using ‘trochanteric flip osteotomy’
- External rotator muscles not divided. The approach must always be cranial to the piriformis muscle.
- Medial femoral circumflex artery (MFCA) protected by intact obturator externus
- Nearly 360° view of femoral head and full 360° view of acetabulum
Relevant Course of MFCA
- The main branch of the MFCA is related to the inferior border of the obturator externus muscle and passes posterior to the femur, towards the intertrochanteric crest.
- It then crosses posterior to the obturator externus and anterior to the triceps coxae (obturator internus and the superior and inferior gemelli).
- Before crossing the triceps coxae, a small branch passes to the greater trochanter.
- The vessel enters the joint capsule between the gemellus superior and the piriformis muscles.
- The trochanteric anastomosis communicates with the ascending branch of the medial femoral circumflex artery at the cranial border of the quadratus femoris.
- Inferior gluteal artery branch, which traverses the inferior border of the piriformis tendon also anastomoses with the ascending medial femoral circumflex artery.
Surgical Technique
1. Position: Lateral decubitus
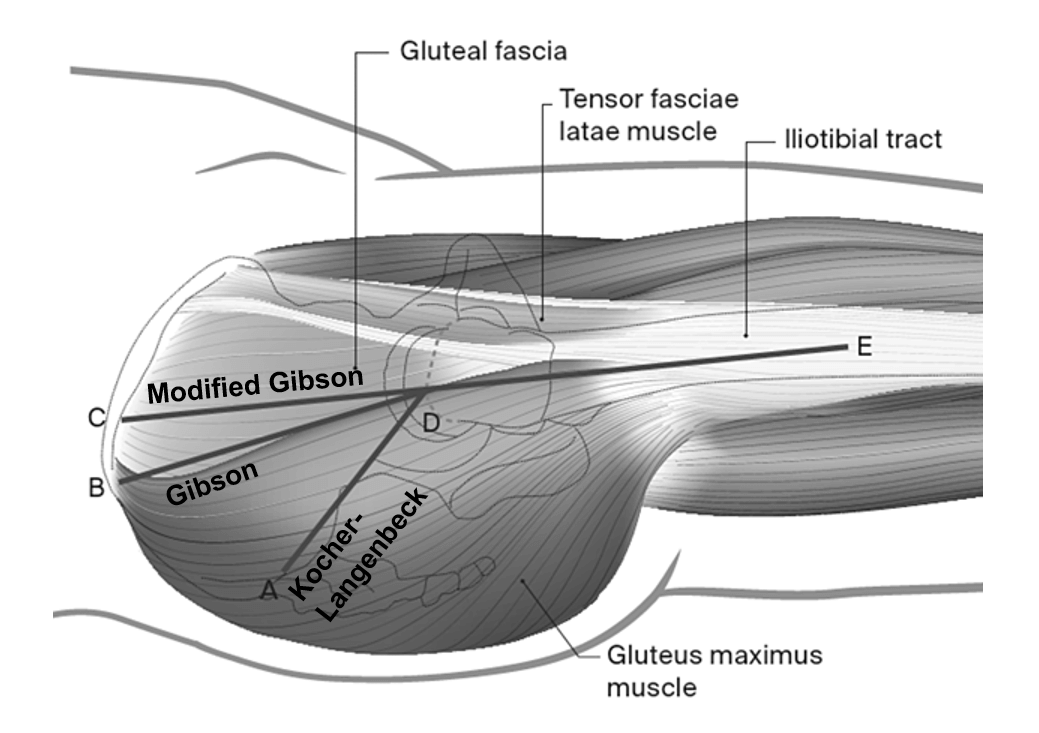
2. Incision and approach: Traditional Kocher-Langebeck (KL) approach or Gibson interval (more anterior interval with posterior retraction of gluteus maximus muscle without violating it)
- Leg is internally rotated to identify posterior border of gluteus medius
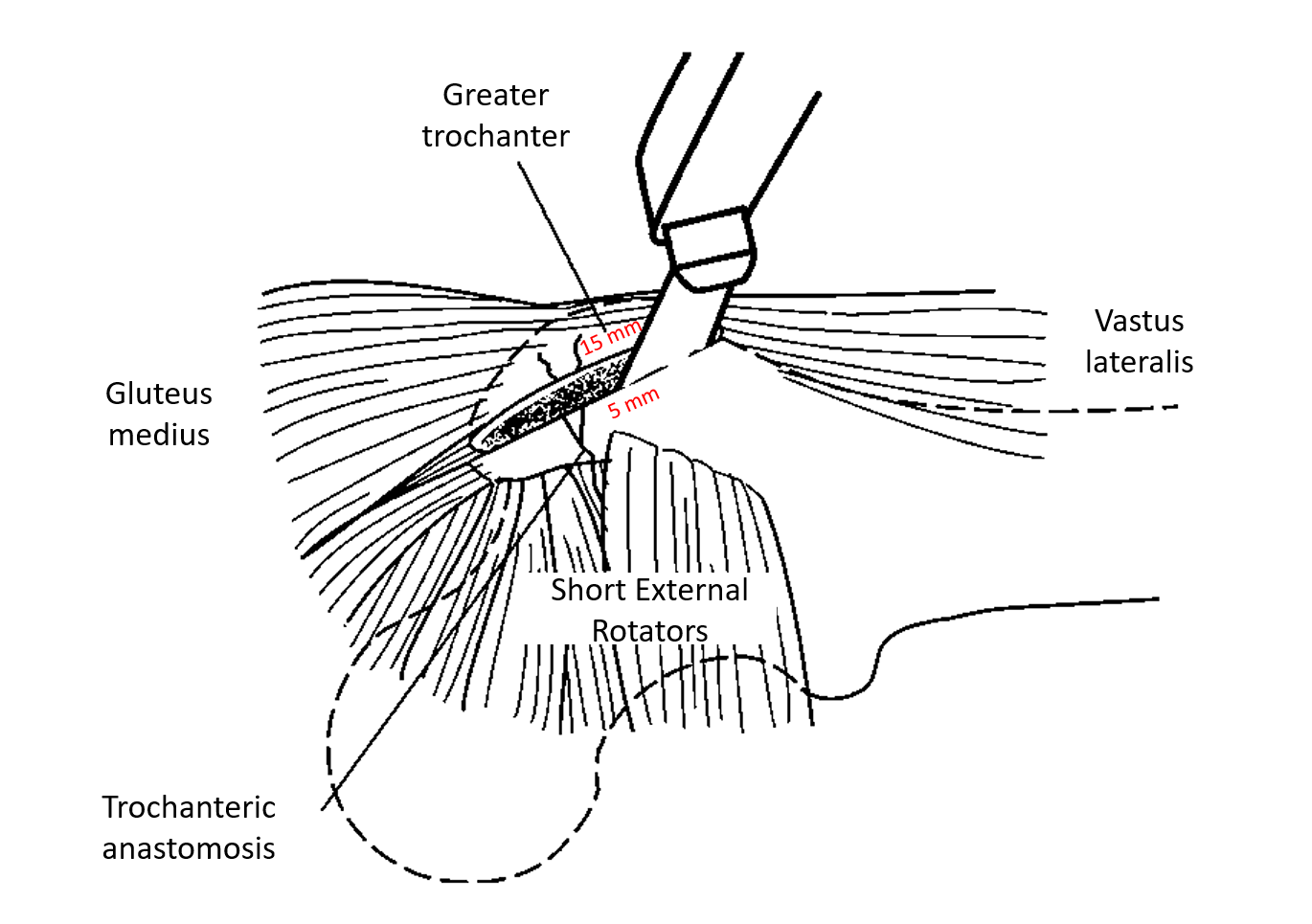
3. Trochanteric (Digastric slide) osteotomy:
- Incision: from posterosuperior edge of greater trochanter to posterior ridge of vastus lateralis.
- Osteotomy: Maximal 1.5 cm thick, exits just anterior to posterior-most gluteus medius insertion.
- leaving all external rotators attached to the stable portion of the trochanter
- Purpose: preserves and protects profundus branch of MFCA
- Trochanteric fragment mobilized anteriorly with vastus lateralis; release posterior gluteus medius fibers as needed.
4. Exposure:
- Flex and externally rotate hip.
- Elevate vastus lateralis and intermedius from anterior femur.
- Retract gluteus medius anteriorly and superiorly to visualize Piriformis tendon
- Inferior border of gluteus minimus is separated from underlying capsule and piriformis (minimus-piriformis interval i.e. gluteus minimus is retracted anteriorly and superiorly; piriformis in retracted inferiorly).
- In double-branched sciatic nerve piriformis muscle is sandwiched between 2 branches and requires the release of tendon from greater trochanter to avoid stretching the branches during dislocation of hip.
- The anterior, superior and posterosuperior capsule can now be visualized.
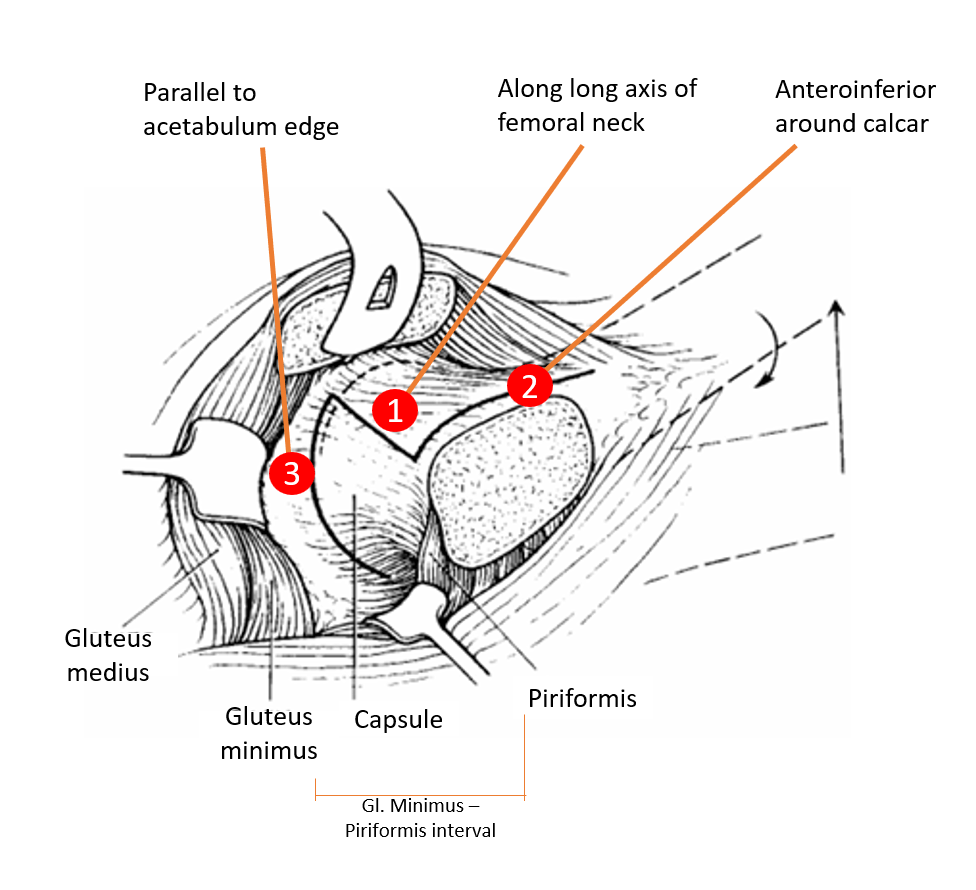
5. Z-shaped Capsulotomy:
- 1st incision: anterolaterally along the long axis of the femoral neck (safe from MFCA)
- 2nd incision: anteroinferiorly (stay anterior to lesser trochanter to protect main branch of MFCA which lies just superior and posterior to lesser trochanter)
- 3rd incision: Extend the 1st incision towards acetabular rim, then turn posteriorly parallel to labrum reaching the retracted piriformis tendon
6. Hip Dislocation:
- Flex, externally rotate, and bring leg over front of table into sterile bag.
- Allows near 360° access to femoral head and acetabulum.
- Ligamentum teres may tear or be incised; foveolar artery is unimportant for head vascularity.
- Inspect sciatic nerve in scarred cases before dislocation.
7. Inspection of acetabulum and femoral head:
- Three retractors for acetabular exposure:
- One above acetabulum
- One on anterior rim
- One levering neck calcar
- No retractors needed for femoral head visualization – adjust leg position.
- Retinaculum (mobile layer of connective tissue) protecting MFCA branches visible on posterosuperior neck.
8. Intraoperative assessment:
- Inspect labrum, femoral head, and acetabulum for pathology.
- Dynamic assessment for impingement possible.
- Therapeutic options: debridement to total hip arthroplasty
- Blood supply check: 2.0 mm drill hole, bleeding from surfaces of cancellous bone after trimming of osteophytes on periphery of femoral head or laser Doppler flowmetry.
- Keep articular cartilage irrigated with Ringer lactate to prevent drying.
9. Closure:
- Reduce hip with traction and internal rotation.
- Capsule repair without tightening (to prevent retinacular vessel tension).
- Trochanter reattachment with 2–3 3.5 mm cortical screws or cerclage wire.
10. Postoperative rehabilitation:
When the quality of bone is good and the patient reliable, the use of two crutches for restricted weight bearing can be limited to 4 weeks.
References:
- Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001 Nov;83(8):1119-24. doi: 10.1302/0301-620x.83b8.11964. PMID: 11764423.
- Pediatric surgical hip dislocation
- Trochanter osteotomy of the acetabulum

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.