Synonyms: Thyroid resection surgery, Thyroid removal surge
Definition: Thyroidectomy is the surgical removal of all or part of the thyroid gland. A “thyroidectomy” should not be confused with a “thyroidotomy” (“thyrotomy”), which is a cutting into the thyroid, to get access for a median laryngotomy, or to perform a biopsy.
Indications:
- Proven neoplasm (FNAC)
- Suspected neoplasm
- Age: Extreme
- Sex: Male
- Hard, irregular texture and fixity
- Hoarseness of voice
- Enlarged cervical nodes
- Recurrent cysts
- Pressure symptoms due to goiter
- Patient’s wish or Cosmesis
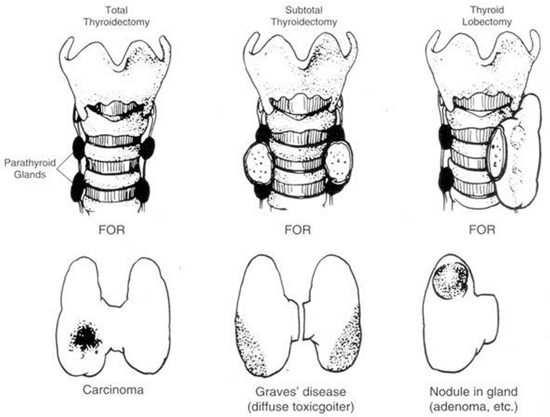
Types of thyroidectomy:
| Thyroidectomy types | Resected parts | Indications |
| Lobectomy or Hemithyroidectomy | Isthmus (Isthmectomy) + 1 lobe of thyroid | Benign diseases of single lobe: a. Recurrent cysts b. Solitary toxic or non-toxic adenoma Minimal Papillary carcinoma (<1 cm, no local invasiveness, no lymph node metastases) |
| Subtotal thyroidectomy | All except about 4 grams of lobe on each side | Toxic multinodular goiter (MNG)
Hashimoto’s disease
|
| Near-total thyroidectomy | All except a rim of thyroid tissue (<1 gm or 1 cm) on one or both sides – saves parathyroid and recurrent laryngeal nerve | Suspicious for malignancies
Malignancies |
| Total thyroidectomy | All | Malignancies (Papillary carcinoma, Follicular carcinoma, Meduallry carcinoma) |
| Completion thyroidectomy | Remnant thyroid tissue following procedures less than total or near-total thyroidectomy. | Malignancy detected on biopsy |
| Hartley-Dunhill operation | Lobectomy on one side + Subtotal thyroidectomy on other side | Non-toxic Multinodular Goiter (MNG) |
Note: Anaplastic carcinoma of thyroid gland is often inoperable. Isthmectomy may be done to relieve the tracheal compression.
Modalities of thyroidectomy:
- Conventional thyroidectomy
- Endoscopic thyroidectomy
- Robotic thyroid surgery
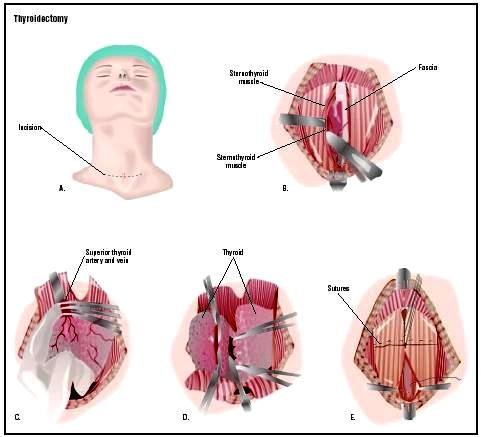
Steps of thyroidectomy:
1. Anesthesia: General anesthesia with Endotracheal intubation
2. Position: Supine with neck hyper-extended by placing a sand-bag under shoulder; table titled to 30° anti-trendelenburg position to reduce venous engorgement
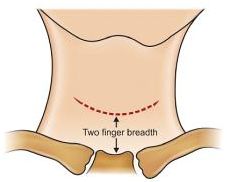 3. Kocher’s thyroid incision: Transverse “collar” incision, 2 finger breadths above the suprasternal notch from one sternocleidomastoid to another
3. Kocher’s thyroid incision: Transverse “collar” incision, 2 finger breadths above the suprasternal notch from one sternocleidomastoid to another
4. Development of subplatysmal plane:
- Skin flaps retracted together with platysma – upper flap raised upto thyroid cartilage and lower flap upto sternoclavicular joint.
- Investing layer of deep cervical fascia is opened longitudinally between strap muscles and between anterior jugular veins.
5. Retraction of strap muscles: Away from thyroid
6. Exposure of thyroid gland: through vertical division of pretracheal fascia
7. Ligation of middle thyroid vein: 1st vein to be ligated
8. Mobilization of thyroid and ligation of vessels in series: Superior followed by inferior
Note: Parathyroids must be identified and Recurrent laryngeal nerve should be identified and saved in Beahr’s or Riddle’s triangle formed by Common carotid artery, Inferior thyroid artery and tracheo-esophageal groove.
9. Division of Berry’s ligament: Separation of isthmus and thyroid lobe from trachea
10. Removal of thyroid: Based on the type of thyroidectomy – the procedure may be repeated on the other side as well
11. Wound closure:
- Reapproximate strap muscles and platysma
- Skin closure with subcuticular stitch
- Dressing
Complications of thyroidectomy:
Intra-operative:
- Anesthetic complications
- Bleeding
- Thyrotoxic storm (in cases of toxic glands)
- Recurrent Laryngeal Nerve (RLN) injury
- Injury to other surrounding structures
Early:
- Respiratory obstruction:
- Hematoma
- Laryngeal edema
- Recurrent laryngeal nerve injury
- Thyroid strom
- Hypocalcemia
- Wound infection
Late:
- Hypothyroidism
- Hypoparathyroidism
- Keloids
- Stitch granuloma

its a good summay