Definition of Puerperium: Period following childbirth during which the body tissues, specially the pelvic organs involute i.e. revert back approximately to the pre-pregnant state both anatomically and physiologically – and lasts 6 weeks or 42 days.
- Immediate: Within 24 hours of childbirth
- Early: Within 7 days of childbirth
- Remote: Within 6 weeks of childbirth
A. Uterus
1. Size
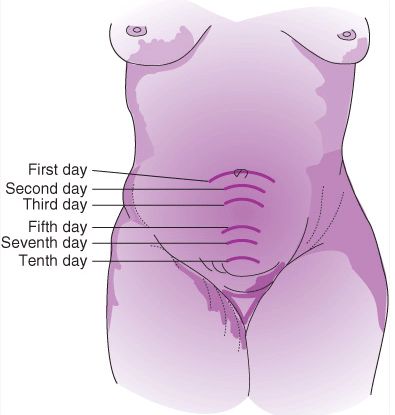
- Just after delivery: 20 cm by length and felt at the level of umbilicus
- ↓ 1.25 cm/day after day 1
- After 1 week: felt midway between symphysis pubis and umbilicus
- After 2 weeks: at the level of symphysis pubis
- By the end of 6th week: 7.5 cm long
2. Weight:
- After delivery: 1000 gm
- By the end of 6 weeks: 50 gm
3. Structure:
- Muscles: Autolysis of excess muscle fibers (number remains same but myometrial cell size decreases) due to increased activity of collagenase and proteolytic enzymes
- Blood vessels: Obliterated by thrombosis, hyalinization and endarteritis/endophlebitis and becomes degenerated – new blood vessels grow inside the thrombi
4. Placental site:
- Within hours: many thrombosed vessels
- Immediately postpartum: size of palm of hand and rapidly decreases in size
- In subinvolution of the placental site: complete obliteration of the vessels in the placental site fails to occur. Patients with this condition have persistent lochia and are subject to brisk hemorrhagic episodes.
5. Endometrial changes:
Within 2-3 days postpartum, remaining decidua becomes differentiated into 2 layers –
- Superficial layer: becomes necrotic, sloughs off as vaginal discharge i.e. lochia
- Basal layer: becomes new endometrium
Regeneration starts by 7th day → Epithelium complete by 10th day → Entire endometrium bu 16th day → Over placental site by 6 weeks
Lochia: Genital tract discharge in the 1st 2 weeks during puerperium – alkaline and composed of blood, decidual fragments, cervical mucus, vaginal transudate and bacteria
- Lochia rubra (red; 1-4 days): consists mainly of blood and decidua
- Lochia serosa (pale; 5-9 days): due to relative decrease in RBC and predominance of leucocytes
- Lochia alba (white; 10-15 daus): consists mainly of leukocytes and mucus
Odor: fishy smell; pH: alkaline (acidic towards end)
Amount: ~ 250 ml for 1st week; Duration: Upto 3 weeks
Significance:
- Malodor: Infection, retained plug or cotton piece in vagina
- Decreased amount: Infection or lochiometra
- Increased amount: Infection
- Persistence of rubra: Subinvolution or retained products of conception
- Duration more than 3 weeks: Local genital lesion
B. Cervix
1. External os contracts slowly (admits only 1 finger by 1st week) – transverse slit like (distinguishing feature from nulliparous os)
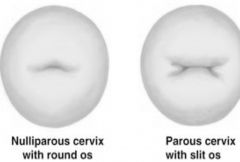
2. Multiparous cervix – characteristic fish mouth appearance
3. Cervical epithelium undergoes much remodeling (~ 50% with high grade dysplasia will show regression)
C. Lower uterine segment
Thinned-out LUS contracts and retracts over a few weeks and forms uterine isthmus
D. Vagina
1. Size: Gradually decreases in size but rarely returns to nulliparous state
2. Mucosa: Remains delicate for first few weeks and submucous venous congestion remains even longer
3. Rugae: Reappear by 3rd week
4. Hymen: Lacerated; caruncle myrtiformes
E. Vulva:
Gaping disappears by the end of puerperium
F. Perineum:
Regains its tone by the end of puerperium while persistence of it’s laxity predisposes to prolapse
G. Peritoneum and Abdominal wall
1. Broad ligaments and round ligaments slowly relax to non-pregnant state
2. Abdominal wall – striae albicans remain
H. Urinary tract
1. Increased capacity and is relatively insensitive to intravesical fluid pressure
2. Retention of urine and predisposition to UTI due to:
- Atony of bladder
- Laxity of abdomen
- Recumbancy
- Reflex inhibition if the perineum is sutured
- Compression of urethra by vulval edema or hematoma
3. Puerperal diuresis (between 2nd – 5th postpartum day): to reverse increased ECF associated with normal pregnancy
4. Dilated ureters and renal pelves return to normal state by 2nd – 8th weeks of postpartum
I. Hematology and Circulation
1. Leucocytosis (upto 25,000/cu.mm) occurs during and after labor
2. Cardiac ouptut:
- ↑ than during pregnancy for ≥48 hours postpartum due to decreased blood flow to the uterus (much smaller) and increased systemic intravascular volume
- By 1 week: blood volume returns to non-pregnant state
3. Hemoglobin and hematocrit: tendency to fall in 1st 2-3 days and return to normal by 8 weeks
4. Fibrinogen and ESR: may be elevated for 2 weeks (risk for DVT)
5. In the first few hours postpartum, an increase in tissue plasminogen activator (t-PA) activity develops, together with a slight prolongation of the thrombin time, a decrease in plasminogen activator inhibitors, and a significant increase in fibrin split products. Protein C is an important coagulation inhibitor that requires the nonenzymatic cofactor protein S (which exists as a free protein and as a complex) for its activity. The level of protein S, both total and free, increases on the first day after delivery and gradually returns to normal levels after the first week postpartum.
6. Platelet decreases soon after placental separation but there is secondary rise with increased adhesiveness (production of both prostacyclin and thromboxane A2 – but shift of balance towards thromboxane A2)
J. Body weight
1. Approach pre-pregnancy weight 6 months after delivery, but still retain ~ 1.4 kg of excess weight
2. 5-6 kg lost by uterine evacuation and normal blood loss
3. 2-3 kg los by diuresis
K. Other General changes
1. Temperature:
- A reactionary rise may occur after difficult labor – doesn’t exceed 38°c and drops within 24 hours
- A slight rise may occur at 3rd day due to engorgement of breasts
2. After pains:
- Painful uterine contractions occur in early puerperium increasing with suckling due to oxytocin release
- Intensity decreases by 3rd postpartum day
- More painful in multipara compared to primipara
3. Breast:
- Colostrum is secreted in the 1st 3 days
- With the establishment of milk secretion at the 3rd or 4th day – breasts become engorged, larger, painful, tender while suckling relieves discomfort
4. Bowel:
- Tendency of constipation due to – intestinal atony, laxity of abdomen and perineum, anorexia and loss of fluids
5. Menstruation:
- Regained by 6-8 weeks after delivery
- Variable period of amenorrhea in lactating women