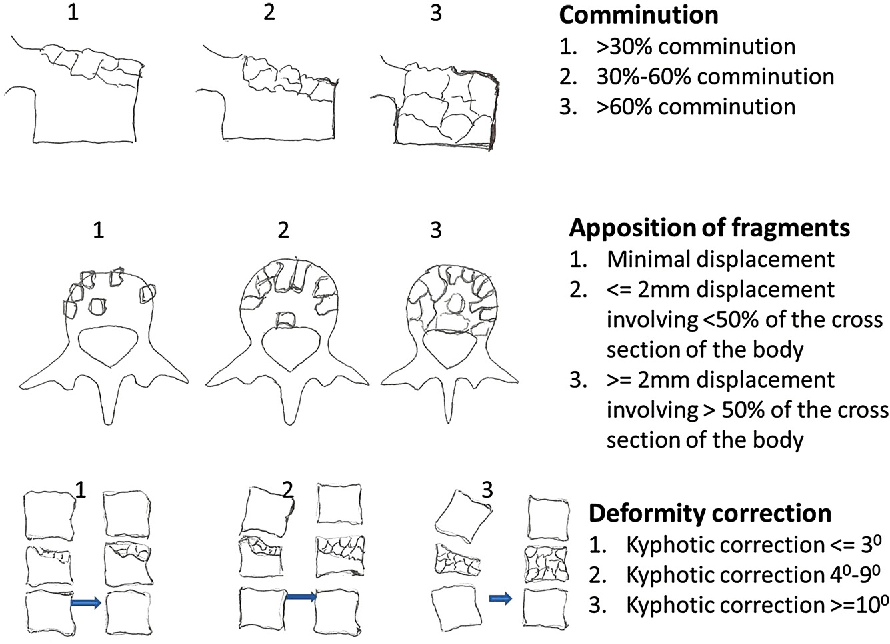
McCormack classification aims to predict the need for anterior stabilization in addition to posterior fixation in cases of thoracolumbar burst fractures. It considers 3 factors for scoring:
- Comminution of vertebral body (best seen on Saggital CT)
- Apposition of fracture fragments (best seen on Axial CT)
- Amount of kyphosis correction in hyperextension (by Cobb’s method in lateral X-ray films)
Principle: Application of load-sharing principle of long bone fixation (load sharing between implant system and host bone) to surgical treatment of acute thoracic and lumbar spine fractures to permit healing and prevent hardware failure –
a. Comminution: Vertebral fragments do not transfer load as well as an intact vertebra
b. Apposition/Displacement: Wider the fracture fragments are displaced, the more poorly they transmit load
c. Kyphosis correction: When severe traumatic kyphosis is corrected, anterior column gap is created eliminating anterior column load sharing and exposing pedicle screw implants to highest possible cantilever bending loads
Interpretation:
- Score ≤6: Short segment posterior stabilization
- Score >6 without dislocation: Anterior instrument and strut graft
- Score >6 with fracture dislocation: Staged surgery; posterior short segment posterior stabilization followed by anterior column support OR Long segment posterior stabilization
Limitations:
Unlike TLICS, this classification system doesn’t incorporate ligamentous or neurological damage and hence cannot be used to assess surgical indication in spine fractures.
The original article was based on the surgical technique of using Stainless steel implant with 4 screws. In the current scenario, all constructs are made of titanium, which is said to have twice the strength and elasticity of stainless steel. Therefore, it can bear more weight and is less likely to break. Modern surgical techniques (like use of intermediate screws at fractured vertebra, cement augmentation at fracture level) and more sophisticated instrumentation may have contributed to the reduction in instrumentation failure.
Modern considerations:
Load-sharing scores up to 6 are 100% reliable, only requiring posterior instrumentation for stabilization. For scores >6, the risk of implant breakage and loss of kyphosis correction in posterior fixation alone is low. Thus, other factors should be considered to define the best surgical approach to be adopted.
References:
- McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures. Spine (Phila Pa 1976). 1994 Aug 1;19(15):1741-4. doi: 10.1097/00007632-199408000-00014. PMID: 7973969.
- Filgueira ÉG, Imoto AM, da Silva HEC, Meves R. Thoracolumbar Burst Fracture: McCormack Load-sharing Classification: Systematic Review and Single-arm Meta-analysis. Spine (Phila Pa 1976). 2021 May 1;46(9):E542-E550. doi: 10.1097/BRS.0000000000003826. PMID: 33273433.
- Stam WT, Deunk J, Elzinga MJ, Bloemers FW, Giannakopoulos GF. The Predictive Value of the Load Sharing Classification Concerning Sagittal Collapse and Posterior Instrumentation Failure: A Systematic Literature Review. Global Spine J. 2020 Jun;10(4):486-492. doi: 10.1177/2192568219856581. Epub 2019 Jun 16. PMID: 32435570; PMCID: PMC7222683.