Anatomy of Umbilical Cord
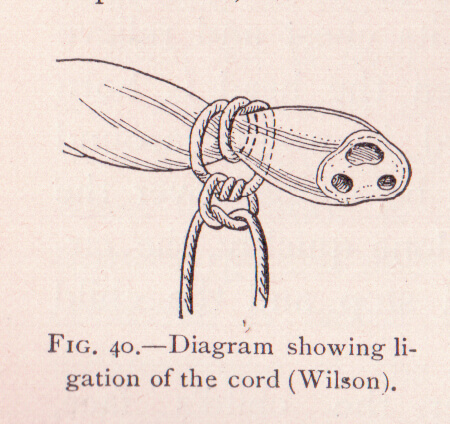
Umbilical cord is a connecting link between fetus and placenta through which fetoplacental circulation occurs. It is formed from allantois carrying vessels from Fetus to Chorion and passing abdominal stalk. It is around 50 cm long and contains 2 umbilical arteries and 1 umbilical vein surrounded by protective Wharton’s jelly. Vessels are arranged in coiled manner and the entire cord appears twisted. Amnion layer coats the cord from the outside. Such configuration like a cord of telephone prevents stress during external compression, stretch or torsion and confers more flexibility to the cord.
Here are various lesions of Umbilical cord seen in Neonates:
Non-coiled umbilical blood vessels
The 3 vessels – 2 arteries and 1 vein are placed in a coiled pattern to form a helical structure within cord. The number of twists can vary from 0 to 40. Left twisted vessels are more common than right. Non-coiled umbilical vessels i.e., untwisted vessels occur in ~ 5% of pregnancies. The structure is identifiable in-utero by ultrasonography (USG).
Non-coiled umbilical blood vessels can be associated with single umbilical artery, trisomy 21 and coarctation of aorta. 10% of such infants are stillborn and there is increased incidence of premature birth.
Single Umbilical Artery (SUA)
Single umbilical artery occurs in 7% of twin births and 1% of single birth. In 1/3 of these babies, gastrointestinal obstructive lesion and urogenital lesions are present. Among the aborted fetuses, studies have found that there is increased incidence of single umbilical artery. There is increased incidence of poor fetal growth and renal anomalies. Therefore, careful physical examination and imaging may be required in such newborns.

Umbilical Granuloma
When the separation of umbilical stump is delayed more than 6 to 8 days after birth, granulation tissue may be formed, which interferes with the epithelialization. The presence of saprophytic organisms delays separation of the cord and increases the possibility of invasion by pathogenic organisms. Mild infection or incomplete epithelialization may result in a moist granulating area at the base of the cord with a slight mucoid or mucopurulent discharge. The tissue is soft, 3-10 mm in size, vascular and granular, and dull red or pink, and it may have a seropurulent secretion. Good results are usually obtained by cleansing with alcohol several times daily. It should be differentiated from everted gastric or intestinal mucosa which permits the entrance of a fine probe Persistence of granulation tissue at the base of the umbilicus is common.
Treatment is cauterization with silver nitrate, repeated at intervals of several days until the base is dry. Sometimes, table salt has been used to treat such condition with success.
Umbilical Polyp
It is a rare anomaly characterized by formation of firm and resistant, bright red structure with mucoid secretion occurring due to persistence of all or part of the omphalomesenteric duct or the urachus. If the polyp is communicating with the ileum or bladder, small amounts of fecal material or urine may be discharged intermittently. Histologically, the polyp consists of intestinal or urinary tract mucosa. Treatment is surgical excision of the entire omphalomesenteric or urachal remnant.
Delayed Separation of Umbilical Cord
When separation of umbilical cord fails to occur after 14 days of birth, the possibility of defect in neutrophil function or chemotaxis should be sought. Leukocyte Adhesion Defect (LAD) is one condition where history of delayed falling of cord is often obtained retrospectively.
Umbilical Sepsis
Umbilical sepsis is superficial infection of the cord characterized by pus discharge, foul odor and induration of the surrounding skin and sometimes, oozing of blood. These are treated with application of gentian violet 1% after cleaning with alcohol spirit. Neomycin powder is also commonly used to treat this condition.

MD Pediatrics and Fellowship Neonatology, he chooses to stay anonymous. He often writes his views online as well as share few important topics for medical students, doctors and specially parents. He does research in pediatrics.