Hernia is classically defined as a protrusion of the contents of a cavity through its walls. It is a condition which occurs not only in the abdomen but also other regions of the body such as in the thorax and cranium. In this article one can find the description of all the types of Hernias except Inguinal Hernia which has been discussed elaborately in another article, link can be found below.
Please go through my two other articles of the Hernia Series before reading further:
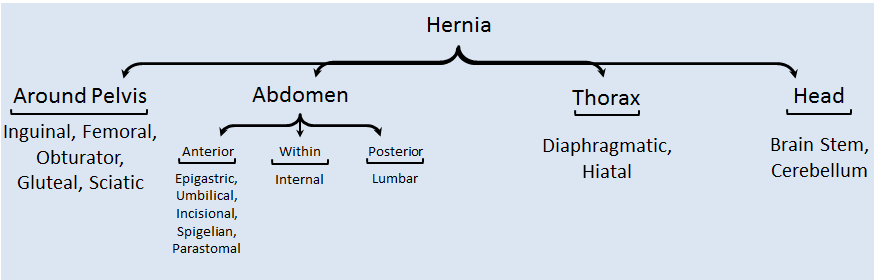
Various types of hernias can be classified based on their location. Inguinal Hernia accounts for the majority of the patients with hernia.
Presentation of a Patient with Hernia & relevant Examination
The patients enter the Clinic with symptoms related to the cavity from which hernia has emerged.
- Lump: Any hernia presents initially as a Lump which is asymptomatic except Spigelian Hernia which remains unnoticeable until the person undergoes some physical examination.
- Pain: Intensity of pain depends upon the cavity. For example, Femoral Cavity has a small opening hence causes more pain compared to others.
- A situation of Intestinal Obstruction may arise in case of Incisional hernia and Internal hernia.
- Reflux: Patients with Diaphragmatic and Hiatal hernia show symptoms of Gastro-Esophageal Reflux.
- Hernia of the contents of the cranium is usually due to increase in Intracranial Pressure, symptoms such as headache, vomiting and blurring of vision may be seen.
- Neuro-Vascular Symptoms: Sciatic hernia may be accompanied with Sciatica (pain radiating along Sciatic Nerve)
- Physical Examination: Swelling is clinically examined traditionally noting the shape, size, consistency, color of the skin, reducibility, pulsation and change in character on cough or Valsalva.
- Any specific symptoms, signs, examination techniques or investigation will be discussed in a relevant area.
Femoral Hernia
Entry of the abdominal contents into the femoral canal (bounded by inguinal ligament, coopers ligament, lacunar ligament and femoral vein) leads to Femoral Hernia. It’s incidence in women is comparatively high than in men. But women still have a higher chance of developing Inguinal hernia than Femoral hernia. Owing to the small diameter of the femoral canal it is common for the bowel loop to get incarcerated and ischemic due to strangulation.
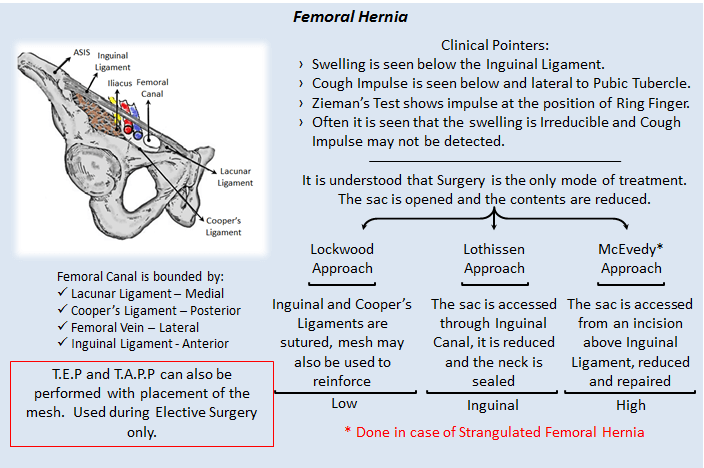
Recurrence may be prevented by suturing Inguinal Ligament to Cooper’s & Lacunar Ligament.
Obturator Hernia
- Obturator canal is present in the pelvis which is formed by the union of the pubic bone and ischium. It is covered by Obturator Membrane through which Obturator vessels and nerves pass through. Obturator hernia is common in women as the canal is wider compared to men.
- It is commonly ignored as the swelling is not significant due to the presence of Pectinius over the sac, but on compression of the Obturator nerve it causes pain in the Antero-Medial side of Thigh (Howship-Romberg Sign) and is relieved by flexion of Hip. It often gets strangulated hence surgery would only be the mode of treatment.
- The sac can be approached from the abdomen or below the inguinal ligament, the sac is reduced by widening or incising the membrane. The defect is closed using a prosthetic mesh avoiding injury to the vessels and nerves. Laparoscopy may also be used but needs to be followed by placing a mesh.
Gluteal and Sciatic Hernia
- These are unusual and do not produce any symptoms until bowel gets obstructed. In Gluteal Hernia the content passes through the Greater Sciatic Foramen either above or below the Piriformis and in sciatic hernia the content passes through the Lesser Sciatic Foramen.
- They only produce a small swelling in the Gluteal region making it unnoticeable, but on compression of the Sciatic Nerve it may cause Sciatic Neuralgia. If Ureter is the content of the sac, Urinary Obstruction may be the symptom.
- As the patient presents with intestinal obstruction or strangulated hernia, Surgery becomes the only mode of treatment where Trans-peritoneal and Trans-gluteal approaches are used to identify the sac which is reduced and the defect is repaired using a mesh.
Umbilical Hernia
- Umbilicus is a portal for the intestines to herniate physiologically during development. After birth in few infants the bowel does not seem to return back to the abdomen and remains outside, it is called Exomphalus.
- Sometimes in premature babies, hernia appears few days after birth, which increases on crying. In such situations truss may be used conservatively and if not fruitful an incision is given just below the umbilicus, the sac is identified and reduced. The sac is excised and defect in linea alba is closed using sutures.
- In adults the contents do not herniate from the umbilicus, whereas they protrude from the area surrounding the Umbilicus and hence termed Paraumbilical Hernia. This occurs due to thinning of linea alba. They contain fat, omentum or bowel depending on the size, but have a very narrow neck and if bowel may become incarcerated or strangulated.
- The main presenting features is swelling, if in becomes strangulated one can experience pain too.
- Small hernia may be left without intervention if they are asymptomatic. Whereas large ones and the ones with strangulation need to be surgically operated.
- Hernia of a small size (<1cm) can be managed by reducing and using a figure of 8 suture.
- Hernia of size <2 cm are incised, inspected, non-viable tissue ligated & excised, sac is removed and the flaps of linea alba are double breasted. This procedure id known as Mayo’s Technique.
- A very large hernia needs the placement of a mesh after the contents are reduced and sac is excised. The mesh can be placed either under the peritoneum, between peritoneum and posterior rectus sheath, between posterior rectus sheath and rectus abdominis or over anterior rectus sheath.
- Alternatively laparoscopic surgery may also be performed followed by placing a mesh.
Epigastric Hernia
- They are midline protrusions on the anterior abdominal wall anywhere between Xiphoid Process to Umbilicus, if present below umbilicus they are named as hypogastric hernia. The contents of the hernia pass through a slit in the Linea Alba (which is a natural opening for small blood vessels). Initially it comprises of extraperitoneal fat hence Epigastric hernia is also known as Fatty Hernia of Linea Alba which later drags out peritoneum and turns into a true epigastric hernia.
- They are usually asymptomatic and only present as a mushroom shaped swelling, but pain may be a complaint if the fat becomes strangulated. It is irreducible and does not expand on cough resembling a lipoma. Rarely, it can present with dyspepsia mimicking peptic ulcer.
- Epigastric hernia is operated only on presenting with symptoms. A vertical or horizontal incision is made and the fat is inspected and pushed in if normal (if infarcted, it is ligated and excised). If peritoneum is found, it is incised and the contents are inspected. If strangulated omentum is fun it is also ligated and excised. The defect in linea alba is closed with non-absorbable sutures.
Incisional Hernia
- Also known as postoperative hernia occurs due to inadequate healing and excess tension of the incision. It is usually seen in conditions such as obesity, chronic cough, inadequate suture technique, wound infection, steroid therapy or malnutrition.
- Incisional Hernia presents as pain and swelling in the region of the previous scar, sometimes as a wound infection too. There may be a discharge oozing out through the scar site (sero-sanguinous). The swelling gradually increases in size and skin over the swelling becomes thin and peristalsis is clearly visible. The neck of the sac is quite broad reducing the chances of incarceration and strangulation.
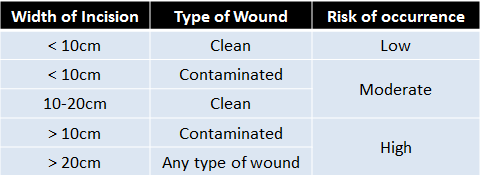
- They can be graded based on the width of incision and type of wound.
- Asymptomatic Hernia can be managed conservatively using an Abdominal Binder. A patent with symptoms needs to be definitely operated.
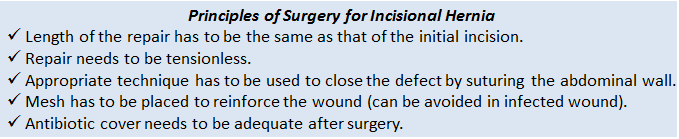
Techniques to close the defect are Mayo’s (double breasting the layers), Keel’s (sac is not opened, bit pushed into the abdomen and pleated with interrupted sutures) or the previous incision is opened sac is identified, incised, reduced, mesh is places and the layers are closed.
Spigelian Hernia/Interparietal Hernia
- This type of hernia remains undiagnosed until a physical examination is done. The abdominal contents protrude through the Spigelian Fascia (between Rectus Abdominis and Transversus Abdominis) till the deep layers of External Oblique hence remain as a small swelling.
- Usually only the extraperitoneal fat herniates leading to symptoms similar to Epigastric Hernia. The opening for the hernia is very narrow which leads to incarceration and strangulation.
- Surgery is commonly done to repair this hernia. A small incision is given over the swelling, sac is identified, incised, inspected, excised and the defect is repaired using sutures. Additionally mesh can also be placed. Alternatively laparoscopic surgery may also be performed.
Parastomal Hernia
- Stoma is an artificial opening created where the bowel is brought out passing through all the musculofascial layers of the abdominal wall. It is a hernia created by the surgeon to serve the purpose of emptying the bowel content. A hernia which occurs through the defect created in the abdominal wall layers is known as parastomal hernia.
- Most of the patients remain asymptomatic, but few show symptoms of strangulation and bowel obstruction. Only such patients are recommended surgical therapy.
- The technique used depends on the patient whether s/he can withstand laparotomy.
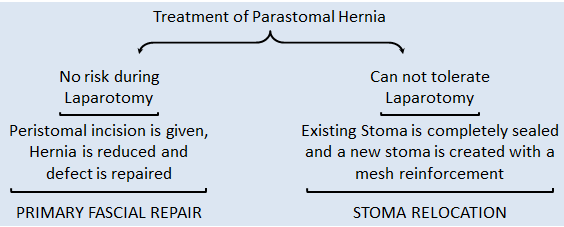
- The ideal surgery is to completely remove the stoma and re-anastomose the bowel which becomes difficult in most of the cases. Though the above two methods described reduce the hernia temporarily, there are instances where hernia reoccurs. Another method to reduce the incidence of parastomal hernia is prophylactic mesh placement during the creation of first stoma.
- Mesh can be places in any of the planes such as intra-peritoneal, retrorectus and onlay using Keyhole (a rent is created in the mesh through which the bowel is passed) or Sugarbaker (the bowel is lateralized and mesh is placed to cover the stoma) techniques.
Umbilical Hernia, Epigastric Hernia, Incisional Hernia, Spigelian Hernia and Parastomal Hernia are grouped under Ventral Herniae.
Internal Hernia
- Internal Hernia is entrapment of a part of small bowel which gets trapped with the defects or openings within the abdomen. It can be caused due to developmental defects or due to operative procedures handling the mesentery.

- They usually lead to strangulation and intestinal obstruction. All the investigations pertaining to intestinal obstruction have to be done and Surgery is the only mode of treatment.
- A laparotomy is carried out to identify the position of intestinal obstruction and the standard principle is to release the constricting agent, inspecting the intestine and repairing the rent. It was later found that presence of vessels and nerves in mesentery made it dangerous to operate, hence another method where the distended loop is decompressed and then the hernia is reduced taking care to avoid contamination of peritoneum.
Lumbar Hernia
- These occur on the dorsal surface of the abdomen through Lumbar triangles or a past surgical scar (Incisional Hernia). There are two lumbar triangles which are formed by different muscles of the back.
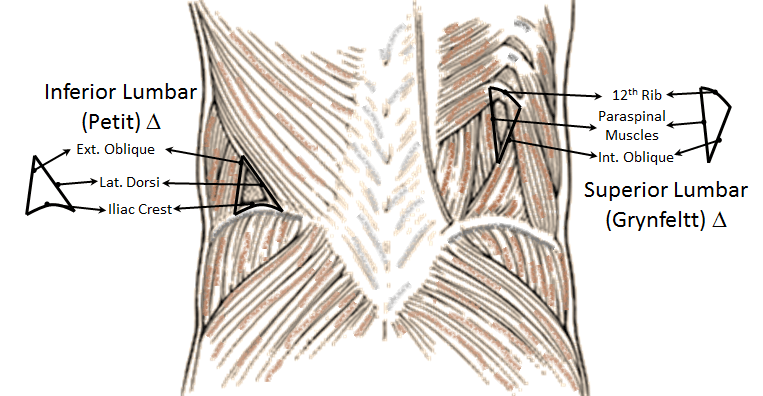
- Lumbar herniae usually are not characterized by symptoms, except when are large. They rarely get incarcerated or strangulated.
- Open or Laparoscopic surgery can be done by identifying the sac, reducing it and placing a mesh.
Diaphragmatic Hernia
- During development of a fetus there is actually no separation between thorax and abdomen, it is just a Pleuro-Peritoneal cavity which becomes a membrane during 8-10 weeks of gestation. This membrane later turns into Diaphragm. This membrane when does not close completely leaves a defect causing the abdominal contents to enter the thorax and compress the developing lung causing pulmonary hypoplasia and pulmonary hypertension.
- Based in the location of the defect, diaphragmatic hernia is od two types:
BochadaLek Hernia – PosteroLateral defect
Morgagni Hernia – AnteroMedial defect
- It may be diagnosed antenatally using an ultrasonogram, if symptoms (chest retraction, cyanosos, grunting and dyspnea) are seen after birth Chest X Ray can detect (intestinal loops in the thoracic cavity).
- At birth the standard resuscitation methods are done which is followed by Endotracheal Intubation and insertion of Nasogastric Tube. Bag Mask Ventilation is absolutely contraindicated. All the necessary fluid and vascular correcting steps have to be continued and Extracorporeal Membrane Oxygenation (ECMO) is provided. If the baby is stabilized, it can be taken up for surgical correction.
- Access is gained through a subcostal incision and the contents are reduced into the abdomen following which the defect is sutured.
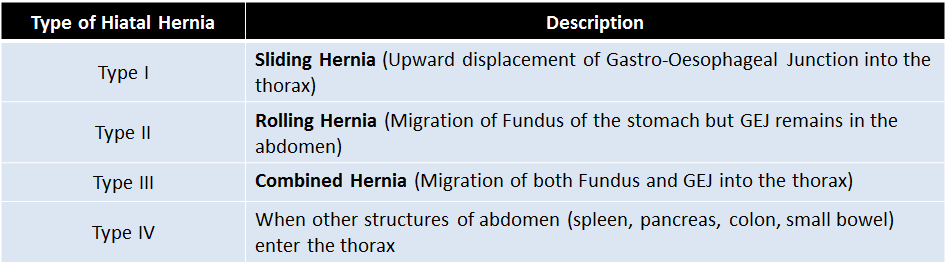
Hiatal Hernia
- When the stomach, spleen, colon or small intestine enters the thorax through the Oesophageal Hiatus in the diaphragm, the condition is known as Hiatal hernia.
- The patient with hiatal hernia presents with symptoms of dysphagia, belching, chest pain, reflux and respiratory discomfort. It may get strangulated and perforated also. CT with oral contrast is the main modality of diagnosis. The standard principles to follow to repair Hiatal Hernia are listed below.
1. Reduction of hernia contents into the abdomen.
2. Excision of hernia sac from the mediastinum.
3. Mobilization of oesophagus into the abdomen.
4. Fundoplication (to prevent reflux).
- During closure of the defect a mesh can also be used in order to reinforce the sutures.
Brain Herniation
- Displacement of cerebrum, cerebellum or brain stem from their anatomical position through natural openings in the cranium such as opening in falx cerebri, tentorium cerebelli or foramen magnum is known as Brain herniation.
- This mainly occurs due to increase Intracranial tension due to various causes such as hydrocephalous, trauma, hemorrhage or mass lesions.
- Patients often reach the Casualty in an unconscious state, when examined they have a low Glasgow Coma Score, pupil become unreactive. Other symptoms are based in the lobe of the brain affected.
- Various types are described such as Uncal herniation, Cingulate herniation, Central herniation and Tonsillar herniation.
- The main aim of treatment is to reduce the intracranial pressure by administering osmotic diuresis (reduce volume of CSF), corticosteroids (reduce swelling), specific surgery to remove the space occupying lesion and craniotomy (to decompress the cranium vault).
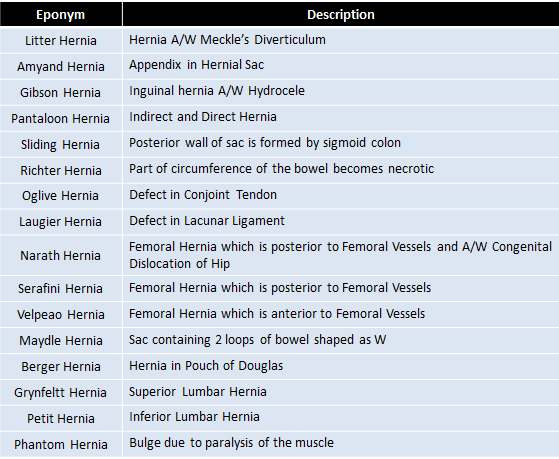
Few Herniae with Eponyms
Summary
Hernia is a well known condition in humans since ancient times, which often lead to mortalities owing to the lack of knowledge regarding the anatomy and the mode of treatment. As time passed by, light was shown onto anatomy and many surgeons put efforts on treating the condition.
Inguinal hernia constitute the majority if the numbers among the patients with hernia. But various other herniae also exist such as femoral hernia, epigastric hernia, umbilical hernia etc.
The basic principle in surgery to treat hernia is to make an incision on the swelling, incise the hernial sac, inspect the sac, reposition the contents in to the cavity (if the contents are ischemic they need to be excised), repair the defect with sutures maintaining tensionless flaps, place a mesh depending on the type of hernia and situation and finally close the layers of the wall of the cavity.
References
- Bailey & Love’s Short Practice of Surgery, 27th Edition.
- Sabiston’s Textbook of Surgery, 20th Edition.
- S. Das’s Concise Textbook of Surgery, 10th Edition.
- Schwartz’s Principles of Surgery, 10th Edition.
- Greenfield’s Surgery Scientific Principles and Practices, 6th Edition.
- Elsevier Saunders’ Surgical Decision Making, 5th Edition.

Graduated from one of the famous institutions in Telangana, Kamineni Institute of Medical Sciences. He has always been fond of writing articles in Medicine. Since the undergraduate years was interested in making creative Presentations and taking seminars.