Special Anatomic Features of Heel Pad
- Heel pad form an almost fully contained cup-like structure consisting of skin overlying a shell of connective tissue within which fibrous septa ramify throughout the heel connecting the underlying periosteum of the calcaneus to the overlying reticular dermis, thereby anchoring skin to bone. Most consistent and significant tether of the heel pad appears to be the medial calcaneal retinaculum.
- Loculi or islands of fat between the septa provide shock-absorbing function.
- The tissue in the heel with the most marginal vascular supply is the relatively avascular fat located in loculi or compartments between the fibrous septa.
- Four arteries supply the heel and form a rich anastomosis with vessels traveling in the fibrous septa between a periosteal and subdermal plexus. However, the septa create relatively avascular compartments of fat which may be vulnerable to ischemia in a scenario akin to compartment syndrome.
- Partial thickness avulsions preserve periosteal blood supply – better prognosis.
- Full thickness avulsions – worse prognosis due to complete loss of blood supply.
6 Angiosomes of Foot and Ankle
a. Posterior tibial artery:
- Calcaneal branch: Medial aspect of ankle and plantar aspect of heel pad region
- Medial plantar branch: Medial aspect of plantar instep, medial 1 and 1/2 toe
- Lateral plantar branch: Lateral aspect of forefoot, plantar aspect of midfoot, and plantar aspect of forefoot, lateral 3 and 1/2 toe
b. Peroneal artery:
- Peroneal artery: Lateral aspect of ankle
- Calcaneal branch: Lateral aspect of heel pad region
c. Anterior tibial artery:
- Dorsalis pedis artery: Dorsum of foot
In healthy subjects, two types of anastomotic arteries create a compensatory pathway between the various angiosomal territories: reduced-caliber (“choke”) and similar-caliber (“true”) anastomotic arteries that provide a redundant conduit allowing a certain angiosome to receive blood from a neighboring angiosome in case of occlusion of the original source artery. The choke vessels demarcate the border of each angiosome.
Classification of Heel Pad Avulsion
Injury can be classified based on laterality and thickness of flap
Order of severity (good to worse prognosis): IA>IB>IC>IIA>IIB>IIC>IIIA>IIIB>IIIC
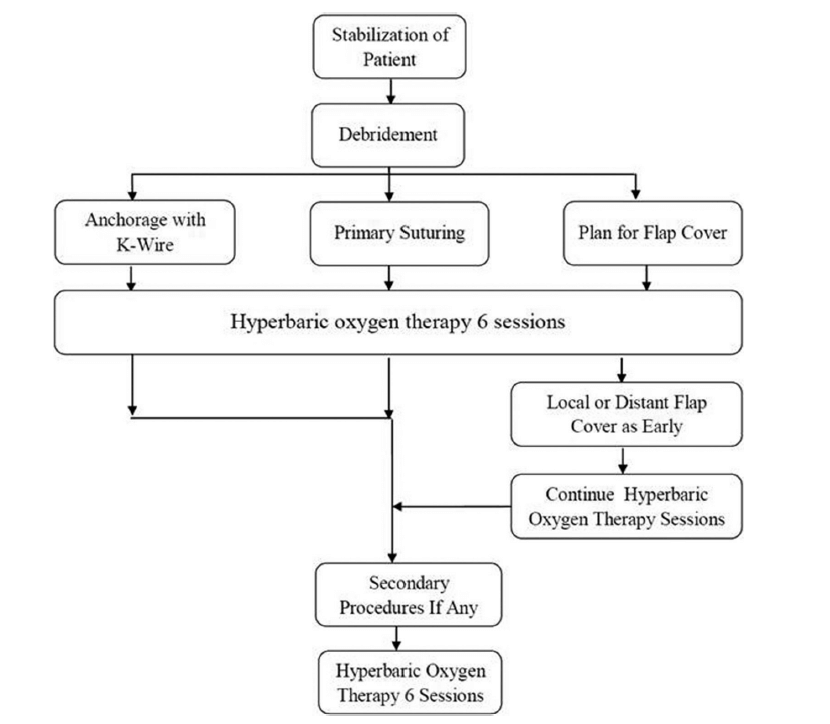
Management of Heel Pad Avulsion Injuries
Aim: to preserve as much viable heel pad tissue as possible and to provide sensate, stable coverage. Principles of wound management with wound evaluation, debridement with preservation of viable tissue, fracture reduction, prevention of infection, and adequate soft tissue reconstruction are important in the management of heel pad avulsion injuries.
References:
- Cichowitz, A., Pan, W. R., & Ashton, M. (2009). The Heel. Annals of Plastic Surgery, 62(4), 423–429. doi:10.1097/sap.0b013e3181851b55
- Snow SW, Bohne WHO. Observations on the Fibrous Retinacula of the Heel Pad. Foot & Ankle International. 2006;27(8):632-635. doi:10.1177/107110070602700812
- http://ota2013annualmeeting.conferencespot.org/55406-otaa-1.2499438/t-001-1.2499977/f-001-1.2499978/a-006-1.2500015/6-1.2500016