Optic disc changes in Glaucoma is one of the most frequently asked topics in Ophthalmology. However, students are often found to have difficulty in understanding and remembering them. Hence, I came up with an idea to illustrate them with schematic diagrams and mnemonics to simplify the topic. The diagrams are conceptual only and may not coincide with the real images.
A. Pathophysiology of Optic Disc Changes in Primary Open Angle Glaucoma (POAG):
- Direct damage by pressure
- Capillary occlusion
- Interference with axoplasmic flow
B. Normal Optic Disc:
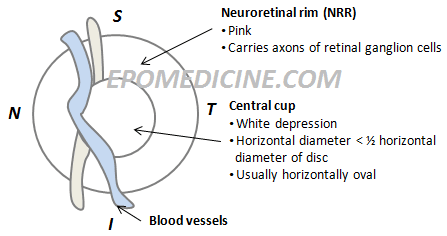
1. ISN’T rule:
- Neuroretinal rim (NRR) is thickest inferiorly
- NRR is thinnest temporally
2. Cup to Disc (C:D) ratio ~ 0.3 to 0.4
3. Asymmetry of C:D ratio in 2 eyes < 0.2
C. Early Glaucomatous Changes:
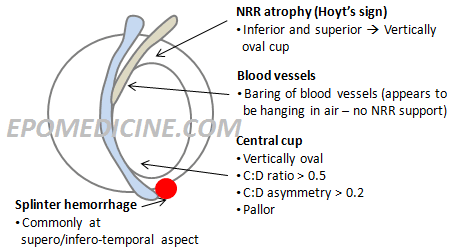
Mnemonic: VLAPS
- Vertically oval cup
- Large cup (C:D ratio > 0.6)
- Asymmetry of cups (Difference of C:D ratio > 0.2)
- Atrophy of NRR
- Pallor areas of disc
- Splinter hemorrhages
Note: ISN’T rule is no more applicable
D. Advanced Glaucomatous Changes:
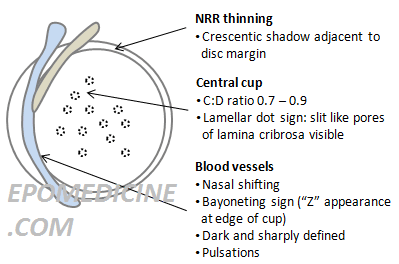
Mnemonic: B-LMNOP
- Bayonetting sign: double angulation of blood vessels
- Baring of circulinear blood bessels
- Laminar dot sign: Slit like pores of lamina cribrosa is visible
- Marked cupping: Cup to disc raio > 0.7 to 0.9
- Nasal shifting of blood vessels
- NRR thinning (Crescentic shadow adjacent to disc margin)
- Optic atrophy: This is the end stage where all NRR are destroyed, Optic Nerve Head (ONH) appears white and is deeply excavated
- Pulsation of retinal arterioles at disc margin
Submitted by:
Sulabh Shrestha

I hypothesize that glaucoma may not an optic disc neuropathy but an axotomy. As the disc/LC sinks the most peripheral fibers being closest to the scleral edge would be first to get stretched and severed followed by next in line central fibers. Severance of nerve fibers would lead to further sinking of the disc(due to loss of anchorage as roots anchor a tree)and thus severance of more of the nerve fibers. This cascade of sinking disc and severance of nerve fibers would continue until the central most fiber is severed in an orderly fashion. End-stage glaucoma disc may not be 100% cupped LC but a crater left over after the severance of all the nerve fibers.