Three sources of Blood supply
- Capsular (retinacular)
- Foveal (ligament of teres)
- Intraosseous
Vascular arragement of Proximal Femur
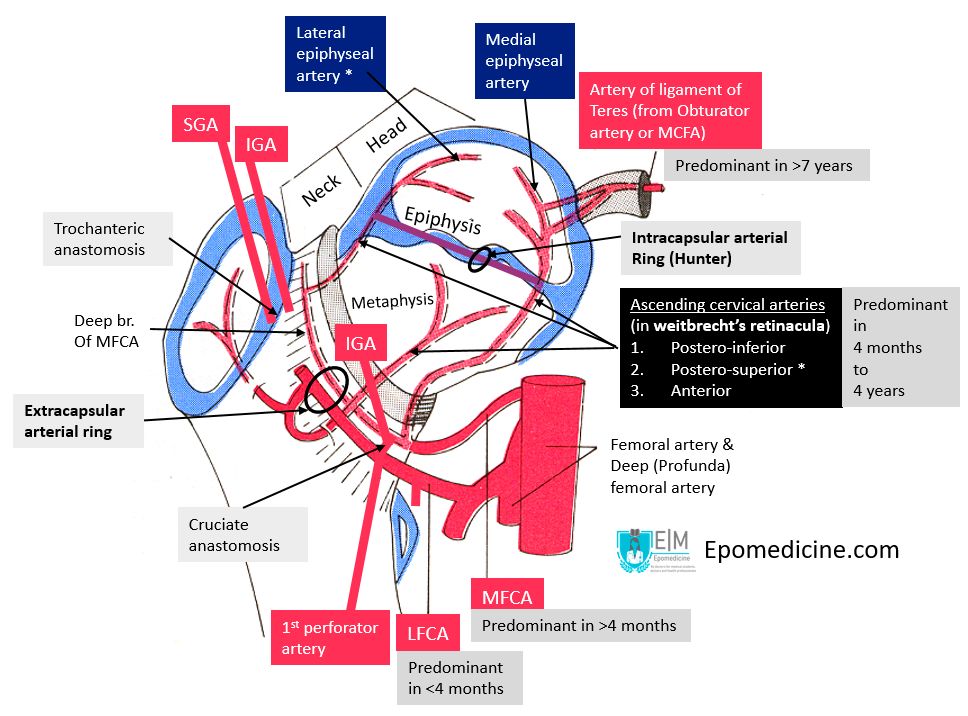
a. Extracapsular ring (At the base of femoral neck)
- Medical circumflex femoral artery (MCFA) – posteriorly
- Lateral circumflex femoral artery (LCFA) – anteriorly
- Minor contribution from: Superior gluteal artery (SGA) and Inferior gluteal artery (IGA)
These circumflex femoral arteries branch from:
- Profunda femoris artery (Deep femoral artery): 79%
- 1 of them from Femoral artery: 20%
- Both of them from Femoral artery: 1%
Trochanteric anastomosis (centered on trochanteric fossa): Descending branch of SGA + ascending branch of LFCA, MFCA and IGA
Cruciate anastomosis (centered on lesser trochanter): Descending branch of IGA + transverse branch of LFCA and MFCA + ascending branch of 1st perforator
Weathersby anastomosis (infra-acetabular region): SGA + IGA + LFCA + Obturator artery (OA)
b. Ascending cervical or retinacular branches (run on femoral neck subcapsularly)
They arise from the extracapsular arterial ring.
They run up in the femoral neck beneath the capsule and gives rise to metaphyseal arteries.
3 groups (4 according to some authors):
- Anterior (from LFCA)
- supplies the femoral neck rather than the femoral head
- Postero-superior (from deep branch of MFCA)
- 80% of foramina are located in postero-superior and antero-superior quadrant of femoral head from where poster-superior group of arteries enter
- most important – can supply entire femoral head without other vascular input
- Postero-inferior (from MFCA)
- 18% of foramina are located in postero-inferior quadrant of femoral head
- As an inferior metaphyseal artery – supplies 2/3rd of metaphyseal head during growth phase
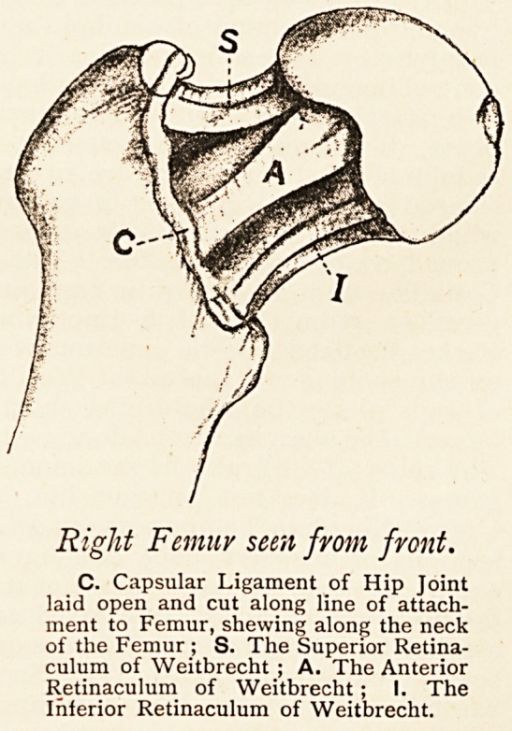
Retinacula of weitbrecht: These are mobile fold of tissue formed by reflections or continuations of the synovial membrane combined with fibrous sheath prolongations of the capsular wall, which carry within themselves the blood vessels of the head and neck. The 3 retinacula are:
- Medial or inferior: constant and strongest
- Lateral or superior: constant
- Anterior: only in 40%
c. Subsynovial intracapsular ring (at the junction of articular surface of femoral head with neck)
Synonym: circulus articuli vasculosus of Hunter
It is more robust on the lateral and medial aspect compared to anterior and posterior aspect.
It can be incomplete increasing the predilection of Legg-Calve-Perthes disease in male gender.
The deep branch of MFCA gives rise to lateral epiphyseal artery which supplies the majority of the femoral head (4/5 th) including the weight-bearing surface is the most important and is particularly prone to injury.
In the absence of deep branch of MFCA, the IGA via the piriformis branch, may be a dominant vessel supplying the femoral head.
d. Artery of ligamentum teres (Enter through fovea capitis)
It usually arises from obturator artery and occasionally from MFCA.
Continues as medial epiphyseal artery – supplies 1/5 of femoral head.
The epiphysis and metaphysis have their own blood supply, and the arteries supporting them during the growth phases are called the epiphyseal arteries and metaphyseal arteries, respectively. In children, the cartilaginous growth plate serves as a barrier to vessels, which do not cross it. The epiphyseal and metaphyseal arteries anastomose after the closure of physis and form intraosseous connection.
Capillary network
The sinusoids found between the trabeculae (inter-trabecular space) are inelastic due to the honeycomb structure with rigid walls of the cancellous bone. Venous congestion can develop from post-capillary blockage from fat emboli due to steroids, alcohol consumption, gaucher’s disease etc. or from disruption of femoral metaphyseal circulation leading to an increase in pressure similar to a compartment syndrome.
Pathophysiology of AVN of femoral head in femoral neck fractures:
- A displaced fracture of the femoral neck will disrupt all intraosseous blood supply leaving only the subsynovial ascending cervical branches and the ligamentum teres.
- The level of the fracture as well as the degree of displacement is important:
- Proximal fractures involving the most superior aspect of the femoral neck almost always disrupt the critical lateral ascending branches.
- More distal fractures may alow the sub-synovial vessels to peel off the neck without being disrupted for displacements of up to 50%.
- If the fracture does not disrupt the capsule of the hip then a haemarthrosis can develop and may cause a tamponade causing a further insult to the vascular supply.
- It is postulated that this increase in pressure is responsible for the albeit low rate of AVN seen in garden 1 and 2 fractures.
Age related changes in femoral head blood supply
The number of lateral and posterior ascending cervical arteries remains constant through maturation, but the number of vessels along the anterior and medial femoral neck decreases by about 50%.
1. Fetal phase (intrauterine life and upto 4 months): Morphologically and functionally LFCA is more developed.
2. Infantile phase (4 months to 4 years): Most intensive collateral development occure between 6 months to 18 months (walking phase). Lateral epiphyseal arteries get stronger and MFCA takes the dominant role.
3. Intermediary phase (4 to 7 years): Epiphyseal arteries are constant while metaphyseal arteries fall behind in development (as epiphyseal plate forms a barrier for metaphyseal arteries). Artery of ligament of teres strengthen during this phase.
4. Prepuberty phase (8 to 10 years): Stabilization of all, already formed anastomosis occurs.
5. Adolescent phase (11 to 15 years): Outer epiphyseal arteries and artery of ligamentum teres are leading the blood supply and are basis for arterial network of the femoral head and neck in adults.
References
1. Zlotorowicz, M., & Czubak, J. (2014). Vascular Anatomy and Blood Supply to the Femoral Head. Osteonecrosis, 19–25. doi:10.1007/978-3-642-35767-1_2
2. Rockwood and Green’s Fractures in Adults, 8th Ed., Volume 1 edited by Charles A. Rockwood, Robert W. Bucholz, Charles M. Court-Brown, James D. Heckman, Paul Tornetta
3. Gojda J, Bartoníček J. The retinacula of Weitbrecht in the adult hip. Surg Radiol Anat. 2012;34(1):31‐38. doi:10.1007/s00276-011-0829-3
4. Ismet Gavrankapetanović, Amel Hadžimehmedagić, Adnan Papović and Mehmed Jamakosmanović (June 28th 2017). Osteonecrosis and Hip Development Disorder, Osteonecrosis, Alessandro R Zorzi and Joao Batista de Miranda, IntechOpen, DOI: 10.5772/intechopen.68161. Available from: https://www.intechopen.com/books/osteonecrosis/osteonecrosis-and-hip-development-disorder
5. Internal fixation of femoral neck fractures: An Atlas edited by Jenó Manninger, Ulrich Bosch, Peter Cserháti, Károly Fekete, György Kazár
6. Pediatric Orthopedic Deformities By Frederic Shapiro

It’s very helpful short and understandable notes. My comment weekly notes if possible