Bilirubin Metabolism
Mnemonic: ABCDE
1. Aged RBCs (80-85%)
- Shunt bilirubin (15-20%): Bilirubin that doesn’t originate from senescent RBCs, i.e. immature or defective RBCs, non-heme compounds (hepatic cytochromes, myoglobin)
- Dyserythropoiesis = Unconjugated hyperbilirubinemia
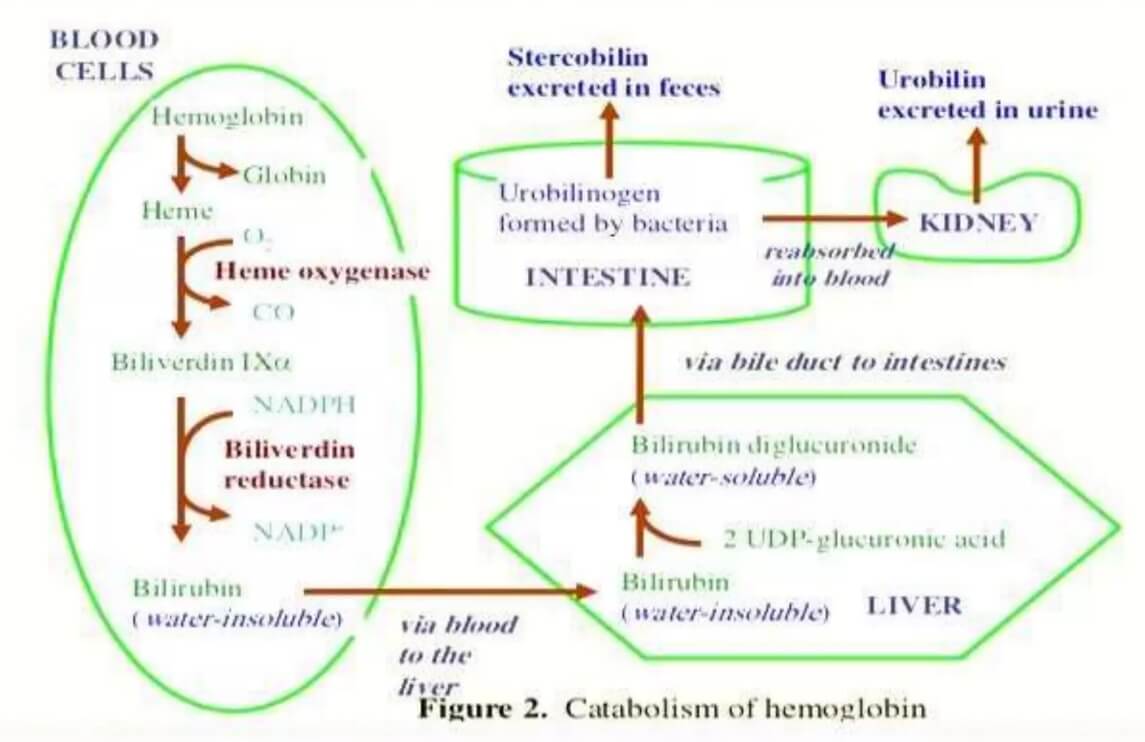
2. Breakdown to Biliverdin and Bilirubin (in reticuloendothelial system)
- RBC = Heme + Globin
- Heme = Iron + Biliverdin (green color)
- Heme-oxygenase enzyme
- Biliverdin = Unconjugated Bilirubin (yellow color; water insoluble; indirect bilirubin)
- Biliverdin reductase
3. Circulation
- Unconjugated bilirubin + Albumin
- Low plasma albumin = Unconjugated hyperbilirubinemia
- Drug competition for albumin = Unconjugated hyperbilirubinemia
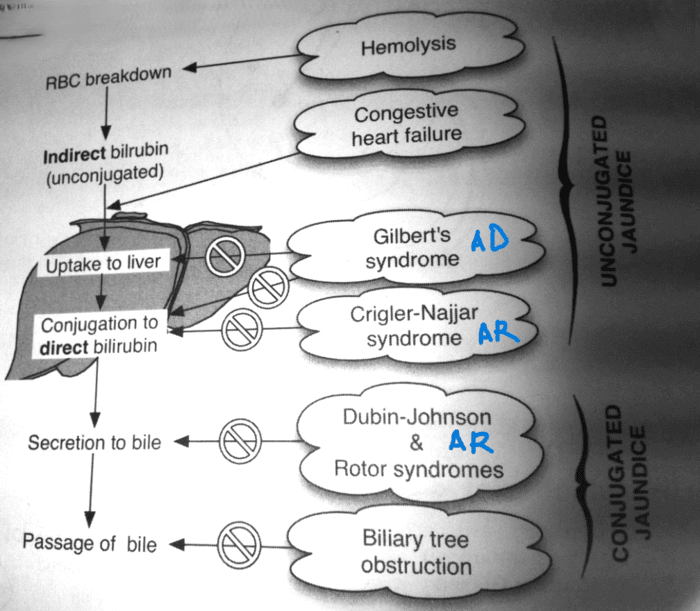
4. Delivery to liver (Conjugation)
- Hepatic uptake of Albumin-Bilirubin complex
- Defect = Gilbert’s syndrome (AD; unconjugated hyperbilirubinemia)
- Unconjugated bilirubin + Glucuronic acid = Conjugated bilirubin (water soluble; bilirubin monoglucuronide 15% + bilirubin diglucuronide 85%)
- UDP-glucuronyl transferase encoded by UGT1A1 (defect = unconjugated hyperbilirubinemia)
- Absence = Crigler Najjar 1 (AR)
- Partial deficiency = Crigler Najjar 2 (AR)
- Reduced activity = Gilbert’s syndrome (AD)
- Slow synthesis after birth = Newborn jaundice
- UDP-glucuronyl transferase encoded by UGT1A1 (defect = unconjugated hyperbilirubinemia)
- Some conjugated bilirubin excreted in urine
5. Excretion and Enterohepatic circulation
- Excessive conjugate bilirubin is excreted in blood and taken up by unsaturated hepatocytes
- Defective OATPB1/B3 transporters = Rotor syndrome (AR; Conjugated hyperbilirubinemia)
- Into bile-canaliculus (Active transport)
- Rate-limiting step
- Defective MRP-2 protein = Dubin-Johnson syndrome (AR; Conjugated hyperbilirubinemia)
- Duodenum
- Terminal ileum and Colon
- Bacterial degradation of conjugated bilirubin = Urobilinogen
- 18% = Enterohepatic circulation (delivered back to liver)
- 2% = Excreted in urine (Urobilin; gives characteristic color of urine)
- 80% = Excreted in stool (Stercobilin; gives characteristic color of feces)
- Bacterial degradation of conjugated bilirubin = Urobilinogen
Unconjugated Vs Conjugated Bilirubin
| Unconjugated bilirubin | Conjugated bilirubin | |
| Van den Bergh reaction | Indirect | Direct |
| Solubility | Water insoluble; Lipid soluble | Water soluble; Lipid insoluble |
| Blood-brain barrier | Cannot pass | Can pass (Kernicterus) |
| Urinary excretion | Not excreted | Excreted |
Stool and Urine Color in Hyperbilirubinemia
| Bilirubin | Urine | Stool | |
| Pre-hepatic | Unconjugated | Normal (urobilin) | Normal (stercobilin) |
| Post-hepatic | Conjugated | Dark (conjugated bilirubin) | Pale (less stercobilin in stool) |
Inherited Disorders of Bilirubin Metabolism
| Gilbert | Crigler Najjar 1 | Crigler Najjar 2 | Rotor | Dubin Johnson | |
| Hyperbilirubinemia | Unconjugated | Unconjugated | Unconjugated | Conjugated | Conjugated |
| Defect | 1. Hepatic uptake of unconjugated bilirubin 2. Decreased activity of UDP glucuronyl transferase | Absent UDP glucuronyl transferase | Partial deficiency of UDP glucuronyl transferase | Defective hepatic uptake and storage of conjugated bilirubin | Defective secretion of conjugated bilirubin into bile |
| Genetic defect | UGT1A1 | UGT1A1 | UGT1A1 | OATP1B1/B3 | MRP-2 |
| Inheritance | AD | AR | AR | AR | AR |
| Liver histology | Normal or Lipofuscin pigment | Normal | Normal | Normal | Dark centrilobular pigmentation |
| Incidence | 6-12% | Very rare | Uncommon | Rare | Uncommon |
| Plasma bilirubin (mg/dl) | ≤3 in absence of fasting or hemolysis; almost all uncojugated | Usually >20; all unconjugated | Usually <20; almost all unconjugated | Usually <7; about half conjugated | Usually <7; about half conjugated |
| Prognosis | Normal | Death in infancy if untreated | Usually normal | Normal | Normal |
| Treatment | Not required | Liver transplant | Phenobarbital | None | Avoid estrogens |
| Other features | ↓ bilirubin with phenobarbital | No response to phenobarbital | ↓ bilirubin with phenobarbital | ↑↑ urinary coproporphyrin (isomer I <80%) | ↑ urinary coproporphyrin (isomer I >80%) |
Mnemonics:
- Dubin Johnson = Dark liver
- Rotor = Red liver (Normal)