Definition of Short Stature
Short stature refers to the height below 3rd Centile or 2 Standard Deviations (-2 SD) or more below the mean height for chronological age and gender for the standard population.
When height is >-3 SD it’s most likely pathological.
Assessment of Short stature
1. Accurate height measurement: using Stadiometer for <2yrs and on Frankfurt plane for older children.
2. Assess height velocity: cm/year
3. Mid-parental height: Estimated Final Height =
- (Ht of father in cm + height of mother in cm + 13 cm)/2 in Males
- (Ht of father in cm + height of mother in cm – 13 cm)/2 in Females
4. Assessment of Body Proportion: Upper segment to Lower segment ratio – Normal, low or high
5. Sexual Maturity Rating: Normal, Delayed or Advanced
Etiological Assessment and Classification of Short Stature
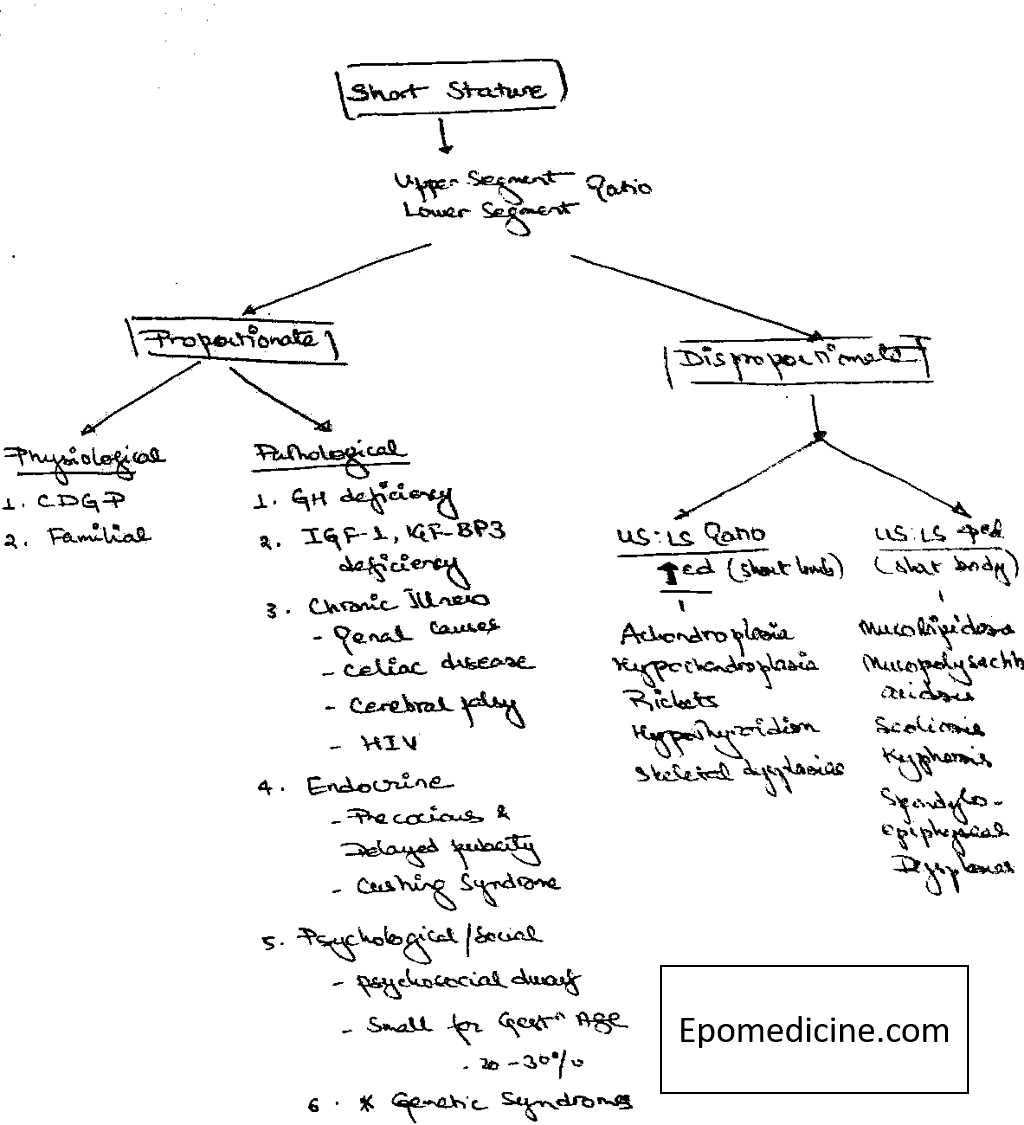
It can be classified on the basis of Upper : Lower segment ratio and then further into Physiological and Pathological causes.
Keeping in mind the causes – history should be sought for Low birth weight, IUGR, Family history of short stature (Achondroplasia, Familial short stature), Delayed puberty and menstruation (CDGP), Bowing of legs and skeletal deformities (Skeletal dysplasias).
Symptoms:
Systemic:
- Renal – Polyuria, Hypertension, Pallor, Hematuria
- CNS – Cerebral palsy
- History of jaundice, white stool, bulky stool
- Recurrent UTI
Neonatal history: hypoglycemia, jaundice, micropenis
Any chronic illness, drug or hormone intake
Social environment
Examination:
- Body Proportions, Skeletal ratios – Rhizomelia, phocomelia, etc.
- Skeletal abnormalities
- Dysmorphism
- Kypho-scoliosis
- Pallor, Hypertension, Jaundice, abdominal distension
- Frontal bossing, depressed nasal bridge, Webbed neck
- Goitre, corase hair
- Central obesity, striae
Evaluation of Short Stature
1. Assess Bone Age and tally with Chronological age: Bone age is assessed by Tanner’s and Whitehouse method or Gruelich-Pyle atlas.
Delayed Bone age compared to Chronological age: All organic cases
a. Bone age proportionate to height age:
- CDGP
- Malnutrition and Systemic Illness-
b. Bone age is less than height age:
- Growth Hormone Deficiency
- Hypothyroidism
- Delayed Pubertry
c. Bone age is Normal for Chronological Age: Familial Short stature
d. Advanced Bone Age:
- Cushing Syndrome
- Precocious Puberty
2. Investigations:
If Height is not below 2 SD: no evaluation – weight and watch 3-6 monthly
If Height <-2 SD, look for SD score:
- If >1 SDS – Physiological varaint
- If <-1 SDS – look for Facies, proportions (if abnormal – Genetic, skeletal dysplasias)
If Normal Proceed with:
- Level I:
- Complete blood count, ESR
- Bone Age
- Renal function test (CKD)
- Urine specific gravity, pH (RTA, CKD)
- Stool RME, Culture, occult blood, pH (GI inflammations, celiac, malabsorptions)
- Liver function test (CLD, Hepatitis, Obstructive jaundice)
- ABG (RTA, Barter and Gittelman syndrome, CKD, Any metabolic acidosis)
- Blood Sugar (GH deficiency, Diabetes type I, Addisons disease, Metabolic disorders)
- Level II:
- Thyroid function Tests
- Karyotyping
- Level III:
- Celiac – TTG for > 2yrs child, Antigliadin Ab for < 2yrs
- GH stimulation assay
- IGF1 and IGF-BP3 assessment
- MRI brain
Management of Short Stature
1. For CDGP and Familial type: Counselling
2. GH therapy for GH deficiency, failure to catch-up, Low birth weight children
GH is currently approved in the United States for treating children with growth failure as a result of Turner syndrome, end-stage renal failure before kidney transplantation, Prader-Willi syndrome, intrauterine growth retardation, and idiopathic short stature.
3. As per pathology for other causes.
References:
1. Nelson Textbook of Pediatrics
2. OP Ghai Essentials of Pediatrics
3. Review articles

MD Pediatrics and Fellowship Neonatology, he chooses to stay anonymous. He often writes his views online as well as share few important topics for medical students, doctors and specially parents. He does research in pediatrics.