Synonyms: Carpal canal
Definition of Carpal Tunnel
Carpal tunnel is an osseofibrous space on the palmar aspect of wrist extending from distal volar wrist crease to the mid-palm, which serves as a passageway to the palm for flexor tendons and the median nerve.
Boundaries of Carpal Tunnel
A. Roof: Flexor retinaculum or Transverse carpal ligament (1-3 mm thick and 3-4 cm wide)
The roof is formed by 3 contiguous segments of flexor retinaculum:
- Thin proximal segment is the deep investing fascia of forearm
- Trasnverse ligament proper originates radially from the tubercle of scaphoid and ridge of trapezium to insert into the pisiform and hook of hamate ulnarly.
- Distal segment is the aponeurosis between thenar and hypothenar muscles.
B. Floor and sides: Palmar radiocarpal ligament and palmar ligament complex between the carpal bones which forms a carpal arch which is concave on palmar side.
Note:
Superficially, the distal volar flexion crease crosses proximal end of scaphoid and pisiform & marks proximal edge of Transverse Carpal Ligament.
Palmaris longus passes in front of the flexor retinaculum to become continuous with palmar aponeurosis.
Ulnar nerve and artery passes above the flexor retinaculum in a separate compartment known as Guyon’s canal.
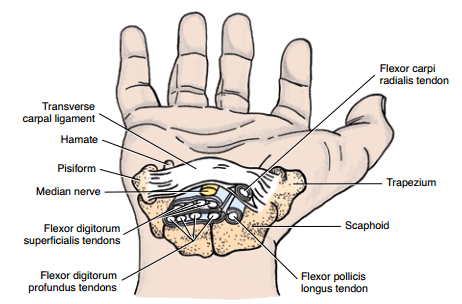
Contents of Carpal Tunnel
A. 9 flexor tendons:
- 4 tendons of Flexor Digitorum Superficialis (FDS) and 4 tendons of Flexor Digitorum Profundus (FDP) in common flexor sheath
- 1 tendon and sheath of Flexor Pollicis Longus (FPL)
Note:
FDS tendons of middle and ring finger are superficial than that of index and little fingers.
1 tendon of Flexor Carpi Radialis (FCR) travels in a separate fascial compartment between two laminae of the flexor retinaculum laterally and is considered by some authors as a content of carpal tunnel.
B. Median nerve:
- Lies most superficially, just beneath the flexor retinaculum
- Reccurent branch supplies LOAF muscles as it passes through the tunnel (Lumbricals – 1st and 2nd, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis i.e. Lumbricals and Thenar group)
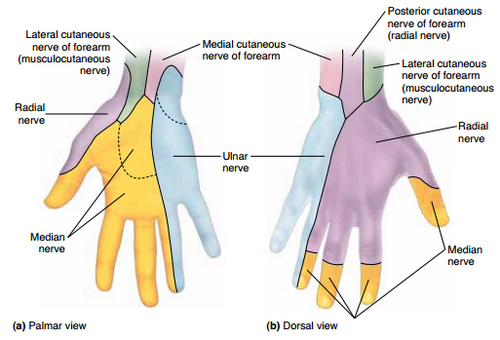
- Palmar digital nerves supply skin of lateral 3 and 1/2 fingers on palmar aspect and only their nail beds on dorsal aspect.
Note:
The palmar cutaneous branch of the median nerve (PCBMN) arises proximal (approximately 5 cm proximal to the wrist crease) to and does not pass through the carpal tunnel; thus sensation in the central palm remains unaffected in carpal tunnel syndrome.
Recently, lumbrical muscle incursion into the carpal tunnel has also been implicated as a possible cause for carpal tunnel syndrome.
Variations exist in the anatomy of median nerve at wrist.
Carpal Tunnel Syndrome (CTS)
CTS results from any lesion that significantly reduces the size of the carpal tunnel or, more commonly increases the size of some of the structures (or their coverings) that pass through it (e.g., inflammation of synovial sheaths). The median nerve is the most sensitive structure in the carpal tunnel. The motor (weakness and wasting) and sensory deficit (paresthesia, hypoesthesia or anesthesia) occurs as described above in the anatomy section.
To relieve the compression and resulting symptoms, partial or complete surgical division of the flexor retinaculum, a procedure called Carpal Tunnel Release (CTR), may be necessary. The incision for CTR is made toward the medial side of the wrist and flexor retinaculum to avoid possible injury to the recurrent branch of the median nerve.
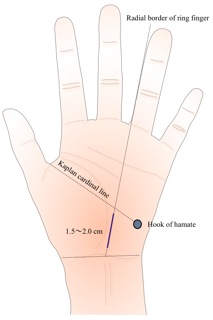
Kaplan’s cardinal line
Kaplan’s cardinal line is a guideline for locating the recurrent motor branch of the median nerve. Recurrent branch is located at the intersection of a line drawn along the ulnar border of the middle finger or radial border of ring finger, with a line drawn between the radial aspect of the thumb web space in abduction and the hook of hamate and pisiform.