Interchangably used as: GIK or GKI regimen.
GKI stands for Glucose, Potassium and Insulin. This simple and effective combined insulin delivery method has gained wide acceptance in perioperative management of diabetic patients who would require Nil Per Oral (NPO) status. Recently, this composition has also been used for management of Acute Myocardial Infarction and Severe Sepsis as well. By supplying glucose, the need for protein catabolism to meet gluconeogenic needs in the diabetic patient is reduced leading to less negative nitrogen balance. Put patient on GIK (Glucose-Insulin-Potassium) regimen according to blood sugar level at least one hour before starting surgery. The GIK regimen should continue at least one hour after the patient has taken the first post operative meal.
Points to remember:
1. A 70 kg person would require 5-10 gm of dextrose per hour
2. 1 Unit of Insulin is expected to lower blood glucose by 25-30 mg/dl
3. Insulin leads to influx of potassium into the cells
4. 1 mmol glucose = 18 mg/dl
5. Target blood sugar is 80-110 mg/dl.
6. Monitor potassium levels every 6 hours.
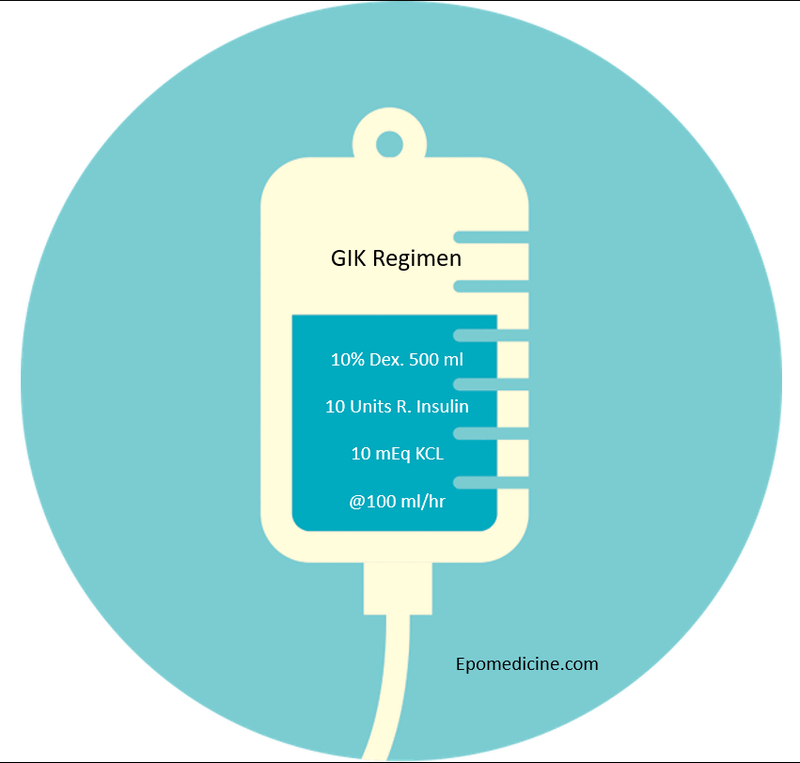
We can remember the original Alberti’s regimen for GIK with the rule of 10 (mnemonic). The GIK regimen is composed of:
1. 10% Dextrose 500 ml
2. 10 Units Short acting (Regular) Insulin
3. 10 mEq KCl
This is started at the rate of 100 ml/hour (i.e. 2 Units/hr of Insulin and 10 grams of Dextrose).
This regimen is for blood glucose level upto 10 mmol (180 mg/dl).
Our target blood glucose is ~ 100 mg/dl.
Capillary blood glucose must be monitored every 1-2 hours on GIK regimen and the concentraltion of insulin must be changed accordingly. For an infusion of separate insulin concentration, a separate bag of GIK regimen must be made.
- For blood glucose between 120-180 mg/dl: Use the same regimen
- For blood glucose below 120 mg/dl: Reduce Insulin by 5 Units (total 5 Units)
- For blood glucose below 80 mg/dl: Stop infusion and administer IV bolus of 50% dextrose in water (25 ml)
- For blood glucose above 180 mg/dl: Add Insulin by 5 Units (total 15 Units)
References:
1. RSSDI Textbook of Diabetes Mellitus By Bb Tripathy, Hemraj B Chandalia
2. Comprehensive Hospital Medicine By Mark Williams, Scott A. Flanders, Winthrop F. Whitcomb, Steven L. Cohn
3. http://medind.nic.in/jac/t00/i3/jact00i3p285.pd
Succinct.
Well written.
Adequate information
Clear picture.
Great job