Synonyms: Accidental hypothermia, Neurotensin-induced hypothermia, Endogenous cryogen-induced hypothermia, Hypoxia-induced hypothermia, Primary hypothermia, Secondary hypothermia
Definition:
The normal body temperature is around 37 c or 98.6 F. Hypothermia is defined as the lowering of core body temperature below 35°C or 95°F.
Classification (Grading):
- Mild: 32°C to 35°C (90°F to 95°F)
- Moderate: 28°C to 32°C (82°F to 90°F)
- Severe: less than 28°C (82°F)
Note: Hypothermia is confirmed by measuring the core body temperature, preferably at two sites. Rectal probes should be placed to a depth of 15 cm and not adjacent to cold feces.
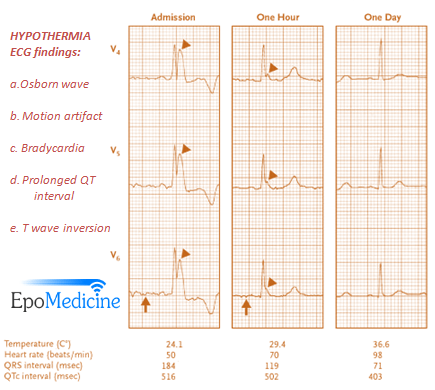
ECG changes and their electrophysiologic basis:
A) Mild hypothermia:
Physiology: Compensatory mechanism supervenes (sympathetic stimulation)
ECG findings:
- Motion (tremor) artifact: Non-specific rapid, intermittent oscillations of ECG due to shivering
- Sinus tachycardia
B) Moderate hypothermia:
Physiology: Prolonged exposure to critically low temperatures will profoundly depress both electrical and mechanical activity in the heart. Systemic vascular resistance falls as catecholamine release is blunted, and cardiac output decreases correspondingly.
In cellular level:
Prolongation of the action potential duration and delayed myocardial conduction has been noticed which can be explained by:
- Delayed activation of the repolarizing potassium current
- Delayed inactivation of the sodium current
- Delayed inactivation of the inward calcium current
ECG findings:
1) Sinus bradycardia associated with progressive prolongation of:
- PR interval
- QRS complex
- QT interval
2) ST elevation or depression and T-wave inversion (acidosis and myocaridal ischemia)
3) Atrioventricular blocks (1st, 2nd or 3rd degree)
4) At temperature below 30°C or 86°F:
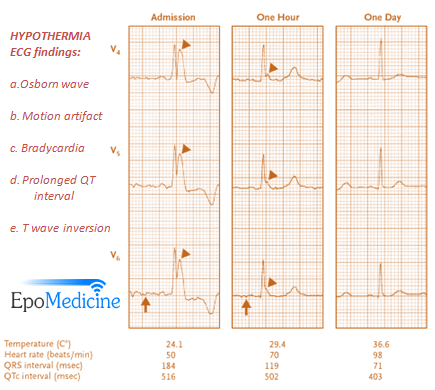
a. Osborn waves:
Synonyms: Camel-hump sign, late delta wave, current of injury, hypothermic wave, K wave, H wave
Not specific to hypothermia: May also occur in hypercalcemia, brain injury, subarachnoid hemorrhage, vasospastic angina, ventricular fibrillation
Defintion: Positive deflections occuring at the junction between the QRS complex and the ST segment, where the S point, also known as the J point, has a myocardial infarction-like elevation
Predominant in: inferior and lateral leads (II, III, aVF, V5 and V6)
Size of J wave: The size of the J waves usually correlates inversely with the body temperature; as the body temperature increases, the J wave gradually becomes smaller.
Suggested mechanism: more prominent transient outward potassium current resulting in a transmural voltage gradient in the epicardium, more pronounced under hypothermic conditions.
b. Atrial ectopics and Atrial fibrillation
C) Severe hypothermia:
Physiology: Ischaemia, increased adrenergic activity and electrolyte disturbances certainly predispose to myocardial irritability which predispose to dyshythmias.
ECG findings:
- Ventricular fibrillation (Secondary to rewarming, hypocapnia, alkalosis or physical manipulation)
- Asystole (Primary manifestation of hypothermia)
Note:
- ECG changes can persist for days after rewarming.
- A hypothermic patient cannot be pronounced dead until rewarmed to normal body temperature.
- Bretylium and Dopamine are the only effective anti-arrhythmic and inotrope in the setting of hypothermia.