Synonym: Hyperpotassemia
Definition: Serum potassium (K+) > 5 mEq/l
Electrophysiologic basis of ECG changes:
In patients with mild hyperkalemia, potassium conductance (IKr) through potassium channels is increased, which tend to shorten the AP duration and on the ECG causing tall tented T waves.
With severe hyperkalemia, effect on RMP becomes prominent. Increased extracellular K+ reduces the Resting Membrane Potential (RMP), i.e. makes it less negative, which leads to partial inactivation of cardiac Na+ channels resulting in slower upstroke velocity of AP. This results in impaired conduction velocity and slowing of AV conduction and intra-ventricular conduction.
a. Atria are more sensitive: Intially, PR prolongation and flattening of P waves
b. Later ventricles involved: QRS widened
c. With extreme hyperkalemia: Total inactivation of Na+ channels and heart stops (cardioplegia)
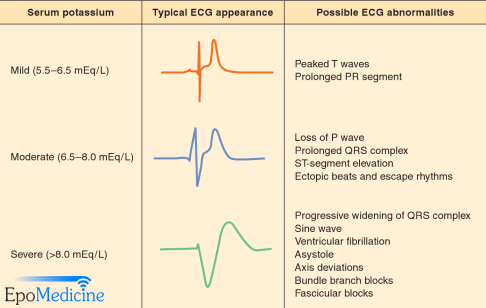
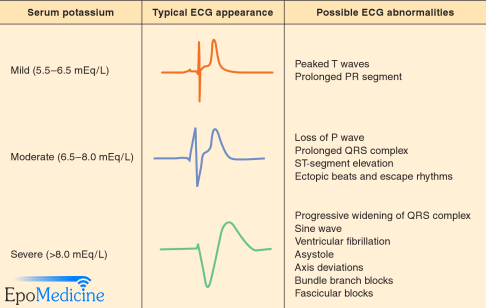
- At K = 5.0 to 6.0 mEq/L, rapid repolarization causes peaked T waves (best seen in leads V2 to V4).
- At K = 6.0 to 6.5 mEq/L, decrease in conduction causes prolonged PR and QT intervals.
- At K = 6.5 to 7.0 mEq/L, P waves are diminished and ST segment may be depressed.
- At K = 7.0 to 8.0 mEq/L, P waves disappear, QRS widens, and irregular idioventricular rhythm appears.
- At K = 8.0 to 10.0 mEq/L, QRS merges with T wave to produce classic sine wave (QRS-T fusion – a sinusoidal waveform).
- At K = 10.0 to 12.0 mEq/L, ventricular fibrillation and diastolic arrest occur.
Note: Hyperkalemia causes tall, peaked (tented) T waves. ECG signs may be absent if the onset of hyperkalemia is slow – as seen in chronic renal failure – even though the serum potassium is in the range of 7 – 7.5meq/L.