Tuning fork
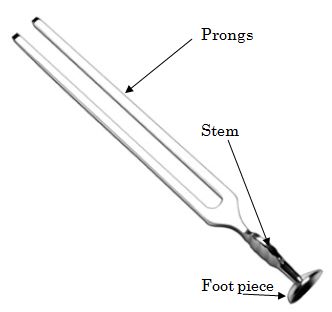
Parts of a tuning fork
1. Foot piece
2. Stem
3. Prongs
How to use tuning fork?
- Hold the stem of the tuning fork between the index finger and thumb of your right hand without touching the prongs.
- Strike the junction of superior 1/3 and inferior 2/3 of the prongs (area of maximum vibration) on a rubber pad or elbow.
Why tuning fork of 512 Hz is ideal for hearing tests?
Tuning forks of lower frequency produce more bone vibration.
Tuning forks of higher frequency have shorter decay time (how fast the tuning fork loses vibratory energy) and are difficult to activate for them to be heard with a moderate or severe sensorineural impairment.
Principle of Air Conduction (AC) and Bone Conduction (BC)
The sound can be transmitted to cochlea in 2 ways:
- Air conduction (AC): Transmission of sound to the cochlea via external air and middle ear
- Bone conduction (BC): Transmission of sound to cochlea via vibration is skull bone, bypassing the external and middle ear.
Since, the cochlear mechanism is same for both the routes, Air conduction (AC) tests the whole ear (conductive and senorineural component) while Bone conduction (BC) tests only the senosrineural component.
Note: Direct transmission of the acoustic signal to the cochlea through the skull vibration is 40 dB to 70 dB less effective than the air conduction pathway. Therefore, in the case of a person listening to air-conducted sound with open ears, bone conduction has minimal contribution to auditory perception.
Tuning fork tests:
1. Rinne test
Principle: Normally, Air Conduction (AC) > Bone Conduction (BC)
Testing Air Conduction (AC): Hold the vibrating tuning fork 2 cm lateral to the test ear, such that both the prongs vibrate parallel to the acoustic axis
Testing Bone Conduction (BC): Hold the vibrating tuning fork and place the foot piece on the flat surface of mastoid just above External auditory canal (not the mastoid tip)
Test for duration:
- Test the BC
- Ask patient to signal as soon as he ceases to hear the sound
- After the patient signals, quickly bring the tuning fork in the position to test AC
- Ask if he can still hear the sound or not?
Test for loudness:
- Alternately test AC and BC
- Ask the patient if loudness of AC or BC is greater?
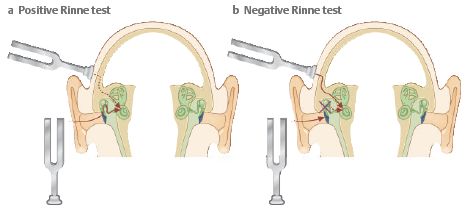
Interpretation:
| Normal | Conductive Hearing Loss (CHL) | Sensorineural Hearing Loss (SNHL) |
| AC > BC (Rinne Positive) | BC > AC (Rinne Negative) | AC > BC (Rinne Positive) |
| Rinne Negative in | 256 Hz | 512 Hz | 1024 Hz |
| Minimum Air-Bone gap | 15 dB | 30 dB (Mild CHL) | 45 dB (Moderate CHL) |
Note: Sometimes, in testing for loudness AC = BC can be noted and this may indicate mild CHL. Test of duration should be performed to confirm.
False Negative Rinne (BC>AC):
This is seen when a patient has severe SNHL on test side and normal hearing on non-test side. On application of vibrating tuning fork to deaf side the sound is transmitted to the non-test ear by bone and patient perceives this bone conduction and presumes that it is perceived by test ear, thus interpreting it as BC > AC.
Associated conditions: Congenital causes, Skull fracture, Meningitis, Mumps, Acoustic neuroma
Correction:
- Masking opposite ear with Barany’s noise box to prevent transcranial transmission of sound
- Weber test is lateralized to better ear
2. Weber test
Principle: This test is useful in identifying unilateral hearing loss. A patient with a unilateral conductive hearing loss (CHL) would hear the tuning fork loudest in the affected ear. This is because the conduction problem masks the ambient noise of the room, whilst the well-functioning inner ear picks the sound up via the bones of the skull causing it to be perceived as a louder sound than in the unaffected ear.
Procedure:
- Place the foot piece or base of the vibrating tuning fork on either of midline of vertex, forehead, chin or upper incisor teeth
- Ask the patient – which ear hears the sound louder?
Interpretation:
| Normal | Conductive Hearing Loss | Sensorineural Hearing Loss |
| Not lateralized (Central Weber) | Lateralized to poorer ear | Lateralized to better ear |
Note: Weber is a sensitive test and a difference of even 5 dB is sufficient to lateralise the Weber.
3. Absolute Bone Conduction (ABC) test
Principle: This is a modified Schwabach’s test where, the bone conduction level of patient is compared to that of the clinician. It includes occlusion of the External Auditory Canal by pressing the tragus to reduce the ambient sound in the surrounding, which is not done in Schwabach’s test.
Pre-requisite: Clinician should have normal bone conduction level or at least he should know his bone conduction level.
 Procedure:
Procedure:
- Examiner closes the test ear by gently pressing the tragus against ear canal.
- Foot piece of vibrating tuning fork is kept over mastoid bone and patient listens to the fork till sound disappears completely.
- Immediately same fork is transferred over mastoid bone of the clinician and simultaneously ear canal is closed by pressing the tragus.
- Clinician listens whether he can appreciate the sound stimulus or not.
- If the clinician doesn’t listen the sound after transferring it from mastoid of the patient, the procedure may be reversed.
Interpretation:
| Test details | Result | Interpretation |
| Clinician listens longer than patient | ABC reduced | SNHL |
| Clinician listens equal to that of patient | ABC normal | Normal |
| Patient listens longer than clinician | ABC lengthened | CHL |
4. Other tests
a. Bing test: This is like ABC test, but the external ear canal is alternately closed and opened by pressing and releasing the tragus.
- Positive bing test (Louder when occluded): Normal or SNHL
- Negative bing test (No change): CHL
b. Gelle’s test: Tuning fork is placed on mastoid and the pressure in the ear canal is increased using the Siegle’s speculum. This increase in pressure in ear canal pushes the tympanic membrane and ossicles inward, leading to rise in intralabyrinthine pressure. This causes immobility of basilar membrane of cochlea, resulting in decreased hearing.
- Positive gelle test (Decreased hearing): Normal or SNHL
- Negative gelle test (Normal hearing): Ossicular chain fixation (otosclerosis) or discontinuation