Synonyms: Pulmonary artery embolism, Pulmonary embolus, PE
Definition: A pulmonary embolus (PE) is a blood clot that embolizes to the lungs. When a clot from peripheral veins, the right atrium or the right ventricle travels into the pulmonary circuit, it effectively blocks forward blood through a portion of the lung bed. If the embolus is large enough to block a major vessel (or multiple vessels), clinically significant signs and symptoms are likely to occur. Fat embolism can occur after orthopedic trauma but air embolism or tumor embolism occur rarely.
Types of Pulmonary Embolism:
A) Based on duration:
- Acute Pulmonary Embolism: Within 48 hours of onset of symptoms
- Subacute Pulmonary Embolism: Symptoms lasting from 48 hrs to 2 weeks
- Chronic Pulmonary Embolism: Symptoms lasting for > 2 weeks (weeks, months or years)
B) Based on size:
- Massive: Occludes >50% of major pulmonary arteries
- Minor: Occludes <50% of major pulmonary arteries
Mechanism of ECG changes in Pulmonary Embolism:
High pressure builds up in the pulmonary circulation proximal to the blockage, and acute strain is placed on the right heart as it tries to pump blood past the obstruction. Due to this acute or subacute rise of pulmonary artery resistance:
- Dilation (not hypertrophy) of the right ventricle and of the right atrium occurs
- Ischemia of right ventricle may occur
- Acute pain, anxiety and hypoxia results in stimulation of sympathetic nervous system
Possible ECG changes in Acute Pulmonary Embolism:
There are about 21 ECG signs associated with PE. These signs may coexist and 10 of the common signs are:
- Sinus rhythm – rate ≥ 90% i.e. may be a normal ECG (80% cases)
- Sinus tachycardia (70% cases)
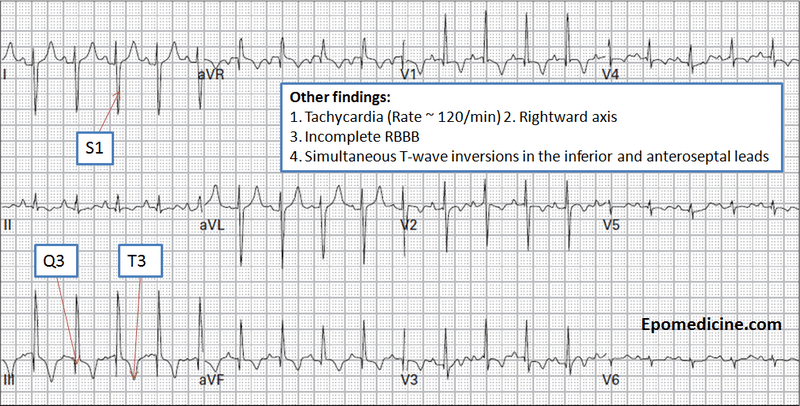
- S1/Q3 pattern or S1/rSr’3 (40% cases)
- S1/Q3/T3 pattern (25% cases)
- Incomplete Right Bundle Branch Block / RBBB (7-60% cases)
- QRS clockwise rotation in precordial leads (35% cases)
- Frontal QRS axis shift to right upto ≥+60° at age >30 years (30% cases)
- R=S in lead V4, V5 or V6
- T negativity: Leads V2 and V3 (30% cases)
- P pulmonale vasculare- atypical (10% cases)
- Tall, Peaked P waves especially in II and V2
- Classical P pulmonale parenchymal rarely seen i.e. ≥2.5 mm in II and purely negative in aVL
- Atrial flutter (5% cases)
- Complete Right Bundle Branch Block/RBBB (3% cases)
Note: RSB = Rechtsschenkelblock = RBBB
Classic Triad of ECG findings – S1Q3T3
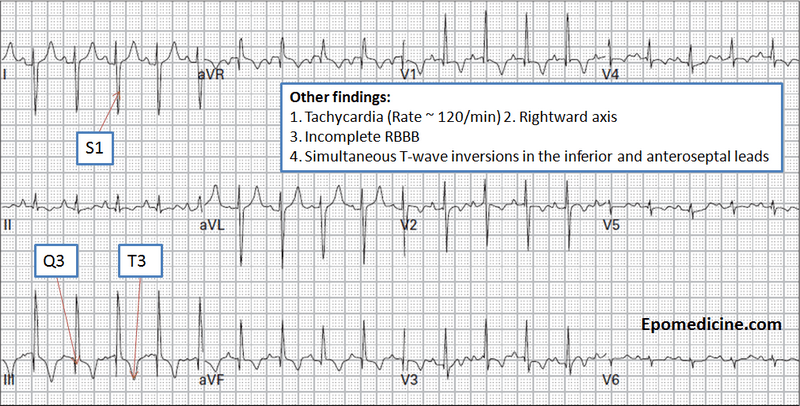
- Synonym: Si/Qiii/Tiii
- Interpretation:
- Deep S wave in Lead I: ≥1.5 mm
- Q wave in Lead III: ≥1.5 mm
- T wave inversion in Lead III
- Neither sensitive nor specific
Reliability: ECG is neither specific nor sensitive for Pulmonary Embolism (PE) but it may one of the first indications of right ventricular overload.
Summary:
1. Have a high index of suspicion: No signs, symptoms, laboratory values, Chest X-ray, or ECG findings are diagnostic of PE or are consistently present.
2. Always keep other causes of Cor pulmonale in differentials
3. Serial ECGs are important in order to accurately diagnose an acute PE
4. ECG findings:
- Commonest is a sinus tachycardia
- Classic triad of ECG – S1Q3T3
- Acute right axis deviation (due to a strain on the right heart)
- Atypical P-pulmonale (vasculare)
- New RBBB
- Sudden ST depression, T inversion or Q in the inferior or anterior leads (simulates ECG signs of myocardial ischemia or infarction)
- Can be accompanied by supraventricular dysrhythmias, including sinus tachycardia, atrial flutter, atrial fibrillation, and paroxysmal supraventricular tachycardia (PSVT)
5. Treatment options: Oxygen, Bed rest, Heaprin therapy, and Thrombolytic therapy

Good explanation!!!