C-spine clearance refers to a clinical decision suggesting the absence of acute bone related, ligamentous and neurologic abnormalities of the cervical spine based on history, physical exam and/or negative radiologic studies.
NEXUS criteria for C-spine Clearance
NEXUS (National Emergency X-Radiography Utilization Study) is a set of validated criteria used to decide which trauma patients do not require cervical spine imaging. Let’s list down the NEXUS criteria with two versions of the mnemonic. Remember either one of these:
Mnemonic: NEXUS
1. Neurologic deficit (focal)
2. Ethanol/Intoxication
3. eXtreme distracting injury (painful injury elsewhere that could distract patient from recognizing the pain associated with a neck injury)
4. Unable to provide history (altered mental status)
5. Spinal tenderness (midline)
Mnemonic: NSAID
1. Neurologic deficit (focal)
2. Spinal tenderness (midline)
3. Altered mental status
4. Intoxication
5. Distracting injury
Note: Presence of any one of these indicates C-spine radiograph and continuing C-spine immobilization.
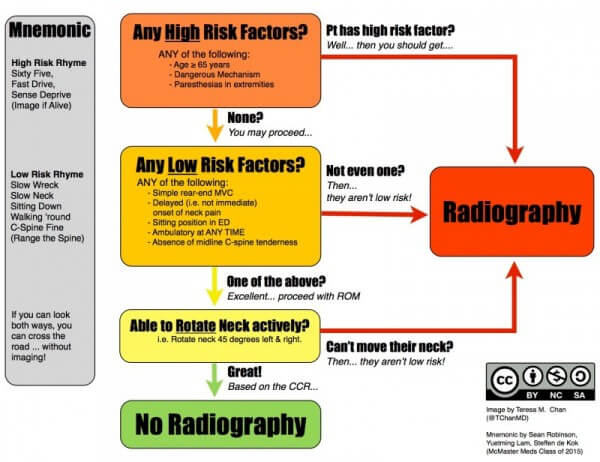
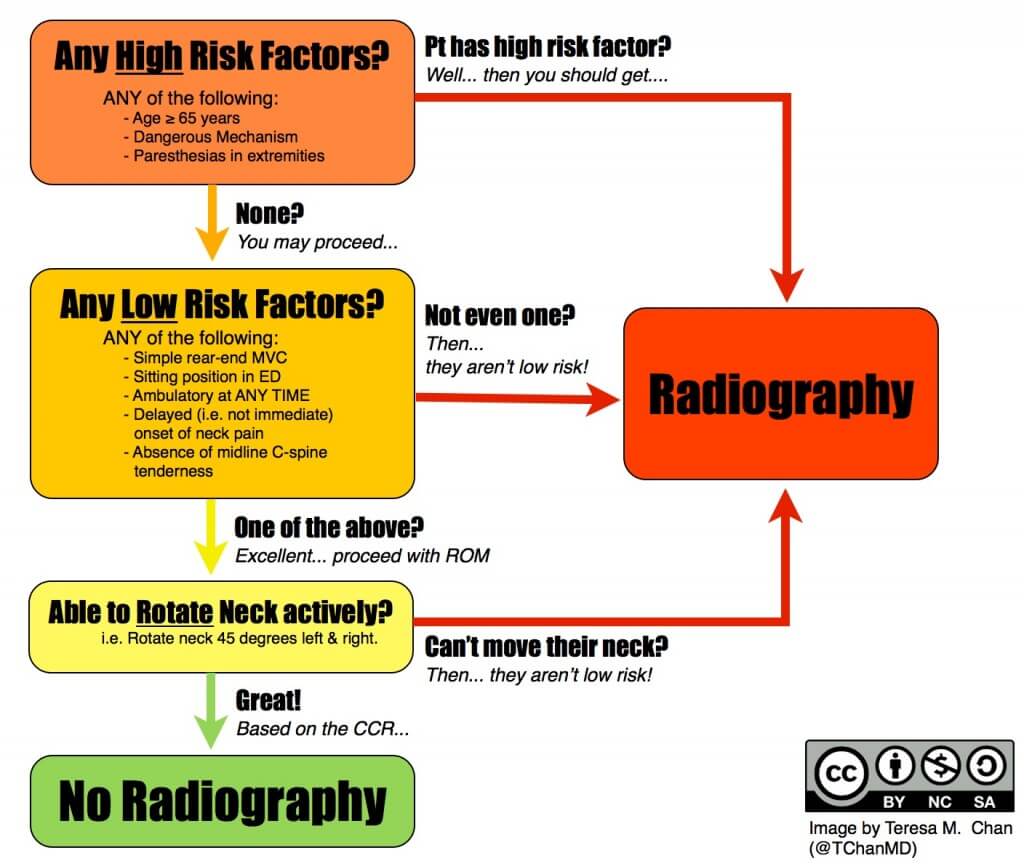
Canadian C-spine Rule (CCR) for C-spine Clearance
Canadian C-spine rule is for alert (GCS 15) and stable trauma patients where C-spine injury is a concern.
Mnemonic:
- High risk features: Sixty five, Fast drive, Sense deprive? Image, if alive
- Low risk features: Slow wreck, Slow neck, Sitting down, Walking around, C-spine fine? Range the spine
- Ultimately: If you can look both wats, you can cross the road without imaging
Fall from elevation ≥3 feet/5 stairs
Axial load to head e.g. diving
MVC high speed (≥100 km/hr), rollover or ejection
Motorized recreational vehicles e.g. ATV
Bicycle collision
Simple rear-end MVC collision:
Pushed into oncoming traffic
Hit by bus/large truck
Rollover
Hit by high speed vehicle
Another mnemonic: MAP65 SLAP45
High risk criteria: Image if any –
- Mechanism – dangerous
- Age ≥ 65
- Paresthesia in extremities
Low risk criteria: Image if any + Able to actively rotate neck to 45 degrees right and left
- Simple rear end collision
- Sitting position
- Late onset neck pain
- Ambulating at any time
- Painless midline neck
For alert patients with trauma who are in stable condition, the CCR is superior to the Nexus criteria with respect to sensitivity and specificity for cervical-spine injury, and its use would result in reduced rates of radiography.
PECARN rule for Pediatric C-spine clearance
PECARN (Pediatric Emergency Care Applied Research Network) provides a basis for risk stratification of children with cervical spine trauma.
Image if any of the following present:
- Altered mental status (GCS <15, AVPU <A, Other findings)
- Focal neurologic deficit (Paresthesia, Loss of sensation, Motor weakness, other findings)
- Neck pain (in >2 years)
- Torticollis (Limited ROM or difficulty moving the neck)
- Substantial torso injury (Thorax including clavicle, Abdomen, Back, Flanks, Pelvis)
- Diving
- High risk motor vehicle crash (Head on collision, Rollover, Ejected from vehicle, Death in same crash, Speed >55mph)
- Predisposing conditions making C-spine more vulnerable to fractures and/or dislocation (Down syndrome, RA, Rickets, OI, Klippel-Feil disease, Ehlers-Danlos syndrome, Achondroplasia, Marfan syndrome, Renal osteodystrophy)