Mnemonic: ABCDEF
For images of the particular Cervical spine (C-spine) X-ray findings and views mentioned below, please refer to the links at the end of the article or use web-search.
Adequacy
- Skull base, C1-C7 and upper T1 must be visible
- 3 views: True lateral, AP, Odontoid (Open mouth) +/- Swimmer’s view (when a standard lateral view cannot image the cervicothoracic junction)
Alignment
There are lines that must run uninterrupted –
- Lateral view:
- Anterior spinal line
- Posterior spinal line
- Spinolaminar line
- Spinous process tips
- Atlanto-occipital alignment: Anterior margin of foramen magnum should line up with dens (clivus point at dens) and Posterior margin of foramen magnum should line up with C1 spino-laminar line
- A normal dens tilts posteriorly and, if it appears straight or anteriorly tilted, fracture should be considered
- AP view:
- Spinous process line (must be in midline)
- Two lateral lines connecting lateral masses
- Odontoid view:
- Line 1: Make sure lateral masses of C1 doesn’t hang over the lateral masses of C2 (rule of Spence: If combined overhang of lateral masses of C1 over C2 on both sides is >6.9 mm – transverse ligament injury making Jefferson or C1 ring fracture unstable)
- Line 2: Make sure there is no asymmetry of the articular spaces between the lateral masses of C1 and the body of C2
- Line 3: Make sure there is no asymmetry of the articular spaces between the dens and the lateral masses of C1
Bones
- Trace outline of each vertebral body – below C2 they must be approximately same height and size
- Crushed vertebral body (burst fracture) or flexion deformity with antero-inferior tear drop (tear drop fracture) are unstable
- Trace outline of each pedicle, lateral mass, lamina and spinous process
- Inspect bone density
- Idenitfy “Coffee Bean” shadow – anterior arch of C1 vertebra always visible on lateral view
- Harris ring: Sclerotic ring formed inside body of C2 by it’s lateral masses (break in the ring outline is suggestive of fracture of peg/body of C2)
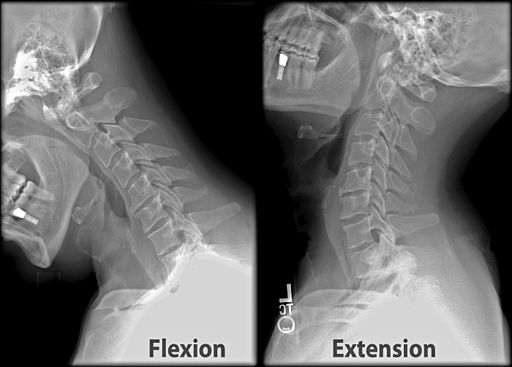
- Flexion views: >11 degrees angulation using end-plate method and >3.5 mm translation between posterior vertebral lines (anterior translation) is suggestive of mechanical instability
- Forward shift of vertebral body: 25% suggests unilateral facet dislocation and 50% suggests bilateral facet dislocation
- Bow tie sign (Unilateral facet dislocation): bodies appear true lateral below level of injury and oblique above level of injury
- Odontoid view may show odontoid fractures which can be classified by Anderson and D’Alonzo classification:
- Type I – Tip (stable)
- Type II – Odontoid base (unstable)
- Type III – Through body of C2 (stable)
- For Basilar invagination:
- McRae’s line: Line drawn from anterior and posterior margin of foramen magnum (basion to opisthion); difficult to evaluate in X-ray
- Chamberlain’s line: Line drawn from posterior margin of foramen magnum (opisthion) to superior margin of hard palate; abnormal if tip of odontoid >3 mm above this line
- McGregor’s line: From superior margin of hard palate to inferior margin of occiput; abnormal if odontoid tip >4.5 mm above this line
Cartilaginous space
- Pre-dental space or Atlanto-dens interval (ADI): space between odontoid peg and anterior arch of C1 (coffee bean)
- Normal in adults: <3 mm (>3.5 mm indicates transverse ligament is damaged)
- Normal in children: <5 mm
- Suggests atlanto-axial instability which can be classified by Fielding and Hawkins classification –
- Type I: Transverse alar ligament intact; odontoid is pivot (rotationally unstable)
- Type II: Transverse alar ligament incompetence; 1 facet is pivot (rotationally unstable)
- Type III: Both facets subluxed anteriorly; ADI > 5mm
- Type IV: Both facets subluxed posteriorly
- Type V: Frank dislocation
Disc and other spaces
- Intervertebral discs: Equal in height at all levels and symmetric and parallel
- Facet joint spaces: Equal distance at all levels
- Spaces between spinous processes:
- C1-C2 space is large
- C3-C7 spaces are similar
- Harris rule of 12: Basion-dental interval (BDI) and Basion-axis interval (BAI) both must be <12 mm (must be </= 8.5 mm on CT)
- BAI = distance from basion to a line tangential through the posterior border of axis (C2)
- Suggestive of occipitocervical dissociation which can be classified by Harborview classification –
- Stage I: <2 mm distraction on traction radiograph
- Stage II: >2 mm distraction on traction radiograph
- Stage III: >2 mm distraction on static radiograph
- Power’s ratio: distance measured from the tip of the basion to the posterior arch of C1 divided by the distance from the opisthion to the anterior arch of C1; >1 is suggestive of occipitocervical dislocation
- Swischuk’s line: A line drawn connecting the anterior cortices of the spinous processes of C1 and C3 should intersect or lie within 1 mm of the anterior cortex of the spinous process of C2. If C2 is >2mm off of this line, it indicates true injury (differentiating from pseudosubluxation)
Double injuries
Discovery of the most obvious lesion is no reason to drop one’s guard as there may be injury at more than 1 level.
Effusion
- Prevertebral space at C2: <7 mm (< 1/3 vertebral body in children above C4)
- Prevertebral space at C6: <21 mm (<1 vertebral body in children from C4 onwards)
A useful mnemonic to remember is: “6 at 2 and 22 at 6”.
Foreign bodies
Any foreign bodies visible in airway tract
Unstable cervical spine fractures:
Mnemonic: Jefferson Bit Off A Hangman’s Thumb
1. Jefferson’s fracture
2. Bilateral facet dislocation
3. Odontoid fracture, type II (through base of odontoid)
4. Hangman’s fracture
5. Atlanto-occipital dissociation
6. Teardrop fracture (flexion teardrop)
Hangman’s fracture can be classified using Levine classification:
Type I – <3 mm displacement, angulation <10 degrees
Type II – >3 mm displacement, angulation <10 degrees
Type IIa – angulation >10 degrees without displacement (DONT GIVE TRACTION)
Type III – bilateral pars fracture and bilateral facet dislocation
Further reading and pictures:
https://dontforgetthebubbles.com/c-spine-x-ray-interpretation/
https://iem-student.org/how-to-read-c-spine-x-ray/
https://geekymedics.com/cervical-spine-x-ray-interpretation-osce-guide/

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.

{kind=link}