- Based on the preoperative clinical examination, the decision on which donor superficialis (FDS) tendon to use is made (commonly FDS middle finger is used).
- Transverse incision is made at the level of the distal palmer crease. Care should be taken to avoid the neurovascular bundles and the flexor tendons must be exposed using sharp dissection.
- The flexor tendon sheaths are exposed from the middle of the metacarpal to the middle of the proximal phalanx.
- The proximal (A1) pulley is identified by its thick, glistening fibrous strands.
- The flexor tendon sheath is opened proximal to the pulley by making a T-shaped incision.
- Distally, the digital fibrous tunnel is opened in an L-shaped incision at the level of the proximal arciform ligament.
- The flexor tendons are identified through the distal opening.
- The flexor digitorum superficialis (DS) tendon of the middle finger is hooked up and cut as distally as feasible without injuring the profundus tendon that lies beneath it. The distal cut end is allowed to retract.
- The tendon is withdrawn through a small curved incision at the base of the palm along the thenar crease.
- The tendon is split into 4 equal longitudinal slips, one slip for each finger.
- The slips are passed deep to the palmar aponeurosis along the flexor sheath with the help of a tendon tunneller.
- The slips are then passed under the proximal pulley of the corresponding finger and through the opening distal to the pulley, and the tendon is taken out and brought palmar to the pulley and proximally.
- Before tensioning the transer, the incision over the base of the palm is sutured as it is difficult once the wrist and MCP joints are in flexed attitude.
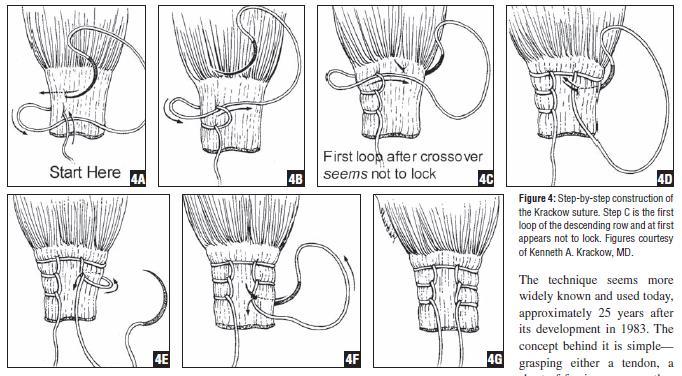
- The slip is sutured to the same slip (thus forming a lasso) under proper tension with wrist in 20° flexion and the metacarpophalangeal joint in about 30-50° to 60-70° (variable according to different literatures) of flexion during tightening (little finger tension is set tighter than the ring finger – maintaining the normal flexor cascade). Additionally, after the tendon transfer is performed, the MCP joint should be able to be passively extended to 0° with some difficulty when the wrist was held in neutral position and with no difficulty when the wrist was flexed.
- Excess tendon slips are trimmed, hemostasis achieved, wound closed and dressing done.
- A dorsal below elbow plaster splint is applied in appropriate position for 3-4 weeks.
Physiotherapy: The aims of preoperative physiotherapy are to keep the skin soft without crack and ulcer, to keep the joint mobile and to increase the strength of the muscle intended for the transfer. The preoperative physiotherapy should be for at least 7–10 days before the surgery and the physiotherapy comprises exercises, oil massage, wax baths, hydrotherapy and splinting. The postoperative physiotherapy usually lasts a period of four weeks during which patients actually learn to use the transferred tendon effectively. They also learn how to protect the new tendon insertion during healing and regain pre-operative range of movements and strengths.
References:
- Gupta V, Consul A, Swamy MK. Zancolli lasso procedure for correction of paralytic claw hands. J Orthop Surg (Hong Kong). 2015 Apr;23(1):15-8.
- Hastings, H., & McCollam, S. M. (1994). Flexor digitorum superficialis lasso tendon transfer in isolated ulnar nerve palsy: A functional evaluation. The Journal of Hand Surgery, 19(2), 275–280. doi:10.1016/0363-5023(94)90019-1.
- Amole IO, Adesina SA, Durodola AO, Adeniran A, Awotunde OT, Eyesan SU. Reconstructive surgical correction of ulnar nerve paralytic claw fingers in Hansen’s disease patients by Lasso procedure. J Case Rep Images Med 2016;2:31–35.
- NARAYANAKUMAR, T. S. (2008). Claw-finger Correction in Leprosy Using Half of the Flexor Digitorum Superficialis. Journal of Hand Surgery (European Volume), 33(4), 494–500. doi:10.1177/1753193408090768.