Synonym: Haemoptysis
Definition of Hemoptysis
Simple definition: Expectoration of blood or bloody sputum
Hemoptysis is defined as the expectoration of blood from the respiratory tract, a spectrum that varies from blood-streaking of sputum to coughing up large amounts of pure blood. 1Harrison’s Principle of Internal Medicine 18e
True hemoptysis is expectoration of blood from the lower respiratory tree, below the glottis. 2Irwin & Rippe’s Manual of Intensive Care Medicine
Classification of Hemoptysis
Hemoptysis has been quantified with different numerical values by different studies and researches.
Massive hemoptysis has been quantified by various studies from as less as 100 ml/day to more than 1000 ml/day. Since, the consensus definition for massive hemoptysis is lacking – let us first define massive hemoptysis:.
a. Expectoration of 100 to 600 ml of blood over 24 hours. 3Harrison’s Principle of Medicine 18e
b. Volumetric: expectoration of 600 ml of blood within 24 to 48 hours; and Magnitude of effect: clinical (hemodynamic and respiratory compromise) 4Irwin’s and Ripple’s Manual of Intensive Care Medicine
c. Expectoration of 600 ml/day or 25 ml/h of blood 5Principles and Practice of Anesthesia for Thoracic Surgery
d. >8 mL/kg/day in children (this reference is widely accepted in pediatrics)
The reason for such a wide variable for quantification may be in part due to the difference in the anatomical deadspace among people. Normally, anatomical deadspace is 100-200 ml and hence, many prefer to use “massive hemoptysis” for expectoration of blood more than 100 or 150 ml/day.
Another, term that has been introduced is the – Exsanguinating hemorrhage which is considered as hemoptysis of:
- >300 ml (in single expectoration)
- >150 ml/hour
- >1000 ml/day
Now, let’s define other spectrum of severity of hemoptysis using a single reference to avoid confusion:
- Mild: <20 ml/day
- Moderate or submassive: 20-600 ml/day 6Textbook of Pulmonary and Critical Care Medicine – SK Jindal, PS Shankar, Dheeraj Gupta
How to Quantify Hemorrhage when Asking the Patient ?
1 tea spoon full (tspf) = 5 ml
1 table spoon full (tbspf) = 15 ml
1 cup ~ 250 ml
Hence, hemoptysis quantified as 1-2 tbspf is generally mild hemoptysis and that >1 cup is usually massive hemoptysis.
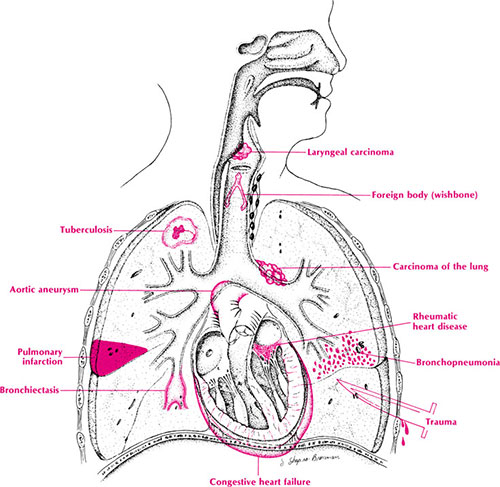
Causes of Hemoptysis
Mnemonic: CAVITATES (remember pulmonary cavitation causes massive hemoptysis)
C – CHF
A – Airway disease, bronchiectasis
V – Vasculitis/ Vascular malformations
I – Infection (eg TB)
T – Trauma
A – Anticoagulation
T – Tumour
E – Embolism
S – Stomach 7PIMP Protector: A medical reference guide for rotations
- Infection: TB, Lung abscess, Bronchiectasis, Pneumonia, Fungal
- Neoplasm: Carcinoma, adenoma, Metastatic
- Congenital: Bronchial cyst, Sequestration of lung
- Traumatic, Iatrogenic, Bleeding disorder
- Cardiovascular: Mitral stenosis, Pulmonary HTN, Aortic aneurysm, AV malformation, PE
- Collagen Vascular Disease: Vasculitis, Wegner’s granulomatosis, Good pasture’s syndrome
Common causes of sub-massive and massive hemoptysis – “3 B”:
- Bronchitis
- Bronchiectasis
- Bronchogenic carcinoma
- Along with Tuberculosis
Hematemesis vs Hemoptysis
| HEMOPTYSIS | HEMATEMESIS |
|---|---|
|
History |
|
|
Absence of nausea and vomiting |
Presence of nausea and vomiting |
|
Lung disease |
Gastric or hepatic disease |
|
Asphyxia possible |
Asphyxia unusual |
|
Sputum examination |
|
|
Frothy |
Rarely frothy |
|
Liquid or clotted appearance |
Coffee ground appearance |
|
Bright red or pink |
Brown to black (acid hematin) |
|
Laboratory |
|
|
Alkaline pH |
Acidic pH |
|
Mixed with alveolar macrophages and neutrophils |
Mixed with food particles |
Pseudo-hemoptysis vs Hemoptysis
Pseudohemoptysis refers to the coughing of blood from a source other than the lower respiratory tract.
Sources of pseudohemoptysis:
- Nasopharynx
- Oral cavity
- Hematemsis aspirated into the lungs
Mechanism or Pathogenesis of Hemoptysis
Understand the vascular anatomy:
Lung has a dual blood supply:
- Low pressure supply (15-20/5-10 mmHg): Pulmonary circulation carries deoxygenated blood from the right ventricle across the pulmonary capillary bed and returns oxygenated blood via the pulmonary veins.
- Supplies pulmonary parenchyma including respiratory bronchioles
- Systemic pressure supply: Bronchial arteries branch from the aorta and are at systemic pressure. They can bleed profusely when airways are diseased.
- Supplies airways (main stem bronchi to terminal bronchioles), pleura, intrapulmonary lymphoid tissue.
- Non-bronchial systemic arteries can also be involved when collateral circulation develops in the regions of chronic inflammation.
Bronchial circulation is responsible bleeding in 90% cases.
Mechanisms involved in various etiologies:
- Neoplasms: Invasion of superficial mucosa and erosion of blood vessels; High vascular tumor with fragile walls
- Pulmonary venous hypertension: High pressure damage venous walls
- Infection: Inflammation and repeated cough disrupts pulmonary vasculature
History taking for Hemoptysis
| Symptoms of upper respiratory or gastrointestinal disease |
| Quantity and rate of bleeding |
| Previous hemoptysis, including extent of previous evaluations Previous history of TB, lung cancer, etc. |
| Appearance of sputum |
| Other pulmonary symptoms (e.g., chronic cough, chest pain) |
| Other systemic symptoms suggesting TB or malignancy (e.g., fever, weight loss) |
| Other bleeding problems and use of drugs (anti-platelet, anti-coagulant) |
| Toxic exposures – cigarette smoke, asbestos, silica |
Aids to Diagnosis Possible Cause of Hemoptysis
Streaky hemoptysis in a tobacco smoker or former smoker over 40 years of age – think chronic bronchitis and possibility of bronchogenic carcinoma.
Remember the most common causes of hemoptysis and massive hemoptysis when evaluating.
Uncommonly think of,
- Monthly hemoptysis – Pulmonary endometriosis
- Cryptogenic hemoptysis (Even after extensive evaluation, a sizable proportion of patients have no identifiable etiology for their hemoptysis) – Dieulafoy disease
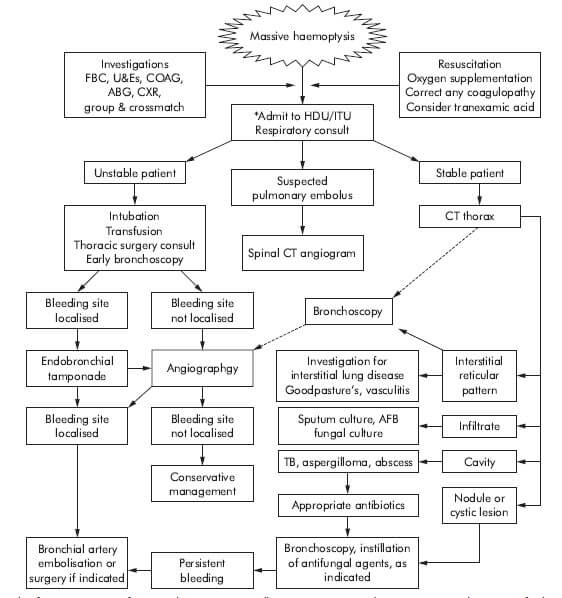
Management of Massive Hemoptysis