
Mechanism of Ethambutol induced optic neuropathy
- Ethambutol is metabolized to a chelating agent.
- The chelating agent formed then may impair the function of metal-containing mitochondiral enzymes, such as the copper containing cytochrome-c oxidase of complex IV and the iron containing NADH:Q oxidoreductase of complex I.
- These mitochondrial respiratory chain play a role in axonal transport in the optic nerves.
- This damage to mitochondrial respiratory chain may lead to development of optic neuopathy.
Ethambutol also has an affinity for the optic chiasm with bitemporal visual field defects manifesting toxicity.
Hamard (1989) believes that optic disc swelling due to ethambutol is the clinical manifestation of a volumetric increase of the neural axons due to blockade of the axoplasmic transport without demyelinating lesions. This concept also explains the improvement after discontinuation of the drug.
EIDOS and DoTS Classification
EIDOS classification is a mechanism classification of adverse drug events.
- Extrinsic species: Ethambutol
- Intrinsic species: Not known
- Distribution: Optic nerve fibers and retinal ganglion cells
- Outcome: Altered physiology initially; later nerve cell degeneration
- Sequela: Optic neuropathy and retinopathy due to ethambutol
DoTS classification is based on time course and susceptibility of adverse drug events.
- Dose-relation: Collateral
- Time-course: Intermediate
- Susceptibility factors: Disease (renal impairment, zinc deficiency)
Dosage and Duration implicated in Ethambutol induced optic neuropathy
Ocular toxicity of ethambutol is dose and duration dependent.
Implicated dose: >25 mg/kg/day
Implicated duration: As early as 1.5 months and as late as 12 months (average 5 months) after initiation of therapy.
Clinical features of Ethambutol induced optic neuropathy
Ethambutol causes optic neuropathy in 1-5% of patients using the anti-tuberculous medication.
Source: Indian Journal of Ophthalmology
1. Dyschromatopsia (earliest feature): Blue-yellow defects, more commonly than red-green defects, may be the initial presentation.
2. Visual acuity: Decrease in visual acuity is insidious and bilaterally symmetrical.
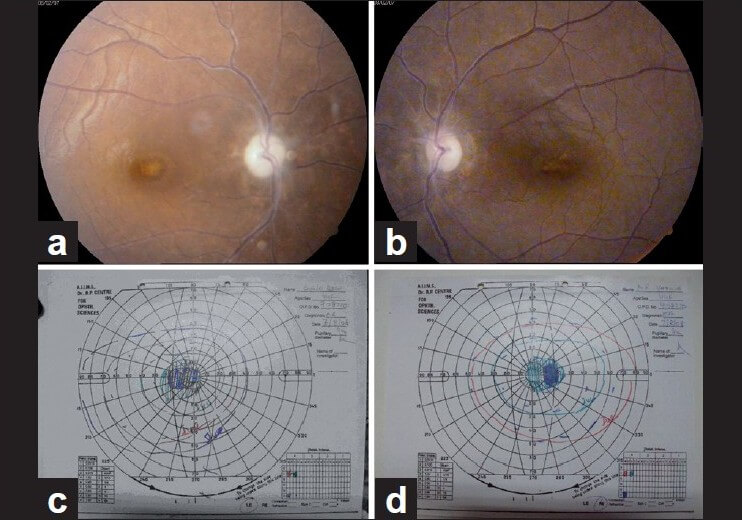
3. Visual field: Typically show central scotomas or bitemporal defects and, less commonly, peripheral constriction.
4. Optic discs: are initially normal but may develop mild temporal disc pallor if ethambutol is continued.
Optic neuropathy, which is primarily retrobulbar, is the most common adverse effect of ethambutol and takes two forms – central and peripheral. The commoner is axial neuritis (central type), which involves the papillo-macular bundle and results in reduced visual acuity, cecocentral scotoma, and blue-yellow color vision impairment. In periaxial neuritis (peripheral type) there is peripheral visual field loss, expecially bitemporal defects, whith sparing of visual acuity and red-green color vision impairment.
Visual acuity, color vision and visual field usually improve slowly once ethambutol is discontinued; however, some patients particularly but not exclusive those in whom optic atrophy has already developed, do not experience an improvement in visual function.
Recommendations
1. Informed consent: Prior to assuming care for patient’s taking ethambutol, explaining that optic neuropathy can occur at any dose despite regular ophthalmologic exams and that the vision loss can be severe and irreversible.
2. Baseline exam: Include:
- Visual field test
- Color vision test
- Dilated fundus and optic nerve exam
- Visual acuity
3. Counsel: Discontinue ethambutol and see an ophthalmologist if any visual symptoms occur.
4. Frequency of examination: For doses >15 mg/kg/day – monthly examination is recommended. Monthly examination at lower doses is recommended in cases of:
- Diabetes mellitus (DM)
- Chronic kidney disease (CKD)
- Alcoholism
- Elderly
- Children
- Other ocular defects
- Ethambutol induced peripheral neuropathy
For others, examination can be done 3-6 monthly.
AOA reccomends weekly home Amsler grid to detect optic nerve involvement.
5. Consider discontinuation: After any signs of loss of visual acuity, color vision or visual field defect.
6. Consider screening for subclinical cases: Ocular coherence tomography (OCT), Contrast sensitivity testing or Visual evoked potential (VEP) may pickup early ethambutol toxicity not detected with the baseline exam.
7. Consider following therapies with unclear significance:
- During ethambutol therapy to limit ocular toxicity: Glutamate antagonists
- Visual signs persist after 4 months of ethambutol discontinuation: Parenteral administration of hydroxycobalamin 40 mg daily over 10-28 weeks
- After diagnosis of optic neuropathy: Oral zinc sulfate 100-250 mg three times daily.
8. Ethambutol in children: Most internation and national guidelines recommend that ethambutol should not be given to children younger than 5 or 7 yearsof age.