
In the chapter of cardiac cycle, we have discussed the mechanism of production of heart sounds and their physiologic splitting.
First Heart Sound (S1)
Mechanism
Closure of atrioventricular valves. It is best appreciated in mitral and tricuspid area of chest for respective components.
Loud S1
Slamming a door from a distance, produces louder sound than slowly closing the door. Also, slamming of door produces louder sound than banging 2 pieces of paper. So, the factors responsible for a loud S1 are:
- Slamming the leaflets in shorter time
- Slamming the leaflets from far apart
- Thicker leaflets
Slamming the leaflets in shorter time: This occurs when the ventricular pressure rises abruptly as in hyperdynamic circulatory states, like:
- Exercise
- Anemia
- Fever
- Thyrotoxicosis
- Pregnancy
- Beriberi
Slamming the leaflets suddenly from a distance: This occurs when ventricular contraction finds atrioventricular leaflets far-apart:
- Short PR interval
Closing the leaflets over longer period from a distance: This occurs when a longer period of ventricular contraction is required to overcome the A-V pressure gradient. This occurs when atrial pressure is higher as in:
- Mitral stenosis
- Tricuspid stenosis
Closure of thicker leaflets: Thickened and stenotic mitral valve
Soft S1
Rigid or Immobile AV valve: Calcified mitral valve
Finding AV valves near during ventricular systole:
- Low A-V gradient: Mitral regurgitation
- Slow rise in ventricular pressure due to decreased contractility: Congestive heart failure
- Long PR interval: Gradually softening S1 in Wenckebach phenomenon (Type I second degree heart block where there is progressive lengthening of PR interval)
Varying intensity of S1
- Atrial fibrillation
- Complete AV block
- Ventricular tachycardia
Wide split S1 (Delayed Tricuspid closure)
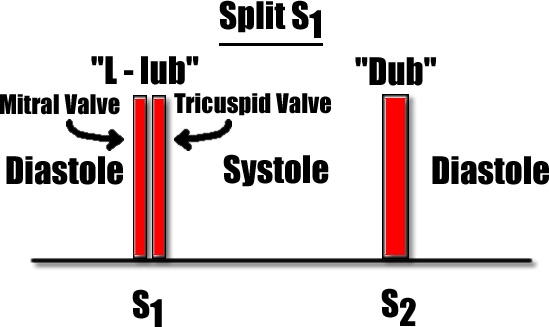
Normally, during inspiration mitral valve closes earlier than tricuspid valve due to increased venous return to right side of heart.
- Electrical impulse reach right ventricle and pressure rises before the same in left ventricle: Right bundle branch block (RBBB)
- Increased venous return to the right side of heart: Atrial Septal Defect (ASD)
- Longer right ventricular contraction needed to overcome high A-V gradient: Tricuspid stenosis
Reversed or No split of S1 (Delayed Mitral closure)
- When electrical impulse reach left ventricle and pressure rises before the same in right ventricle: Left bundle branch block (LBBB)
- Longer left ventricular contraction needed to overcome high A-V gradient: Severe mitral stenosis
Second Heart Sound (S2)
S2 is usually louder than S1 at the heart’s base and usually slightly higher in pitch than S1 at the heart’s apex. It has 2 components:
- Aortic component (A2)
- Pulmonic component (P2)
Mechanism
Closure of semilunar valves. It is best appreciated at the pulmonary area or Erb’s point in the chest.
Intensity or Loudness of A2 and P2
Intensity of S2 is directly related to the closing pressure in the aorta and pulmonary artery. Since, the pressure is much higher in the aorta, normally A2 is louder than P2.
Loud A2:
In conditions of elevated aortic diastolic pressure.
- Essential hypertension
- Syphilitic aortic regurgitation
- Hyperdynamic circulatory states
Soft A2:
- Aortic stenosis
- Aortic regurgitation
Loud P2:
In conditions of elevated pulmonary artery diastolic pressure.
- Pulmonary hypertension
- Mitral stenosis
- Heart failure
Soft P2:
- Pulmonary stenosis
- Pulmonary atresia
- Tetralogy of Fallot
Wide mobile splitting of S2 (During Inspiration only)
Delayed electrical activation of right ventricle:
- Right bundle branch block
- Ectopic from left ventricle
Prolonged right ventricular systole:
- Pulmonary stenosis
- Pulmonary hypertension
- Massive pulmonary embolism
Early aortic closure:
- Mitral regurgitation
Reversed (Paradoxical) splitting of S2 (During Expiration only)
Delayed electrical activation of left ventricle:
- Left bundle branch block
- Ectopic from right ventricle
Prolonged left ventricular systole:
- Systemic hypertension
- Severe aortic stenosis
- Hypertrophic cardiomyopathy
- Patent Ductus Arteriosus (PDA)
- Severe left ventricular dysfunction
Early pulmonary valve closure:
- Tricuspid regurgitation
Early electrical activation of right ventricle:
- WPW syndrome
Wide Fixed Splitting of S2 (Both Inspiration and Expiration)
Right sided volume overload irrespective of inspiration or expiration:
- Atrial Septal Defect (ASD)
- Severe right ventricular failure
Single S2
- Absent or markedly attenuated A2: Severe aortic stenosis
- Absent of markedly attenuated P2: Severe pulmonary stenosis
- Tetralogy of Fallot