
Wilm’s tumor is the most common primary renal tumor of childhood.
Origin: Embryonic nephrogenic (mesodermal) cells
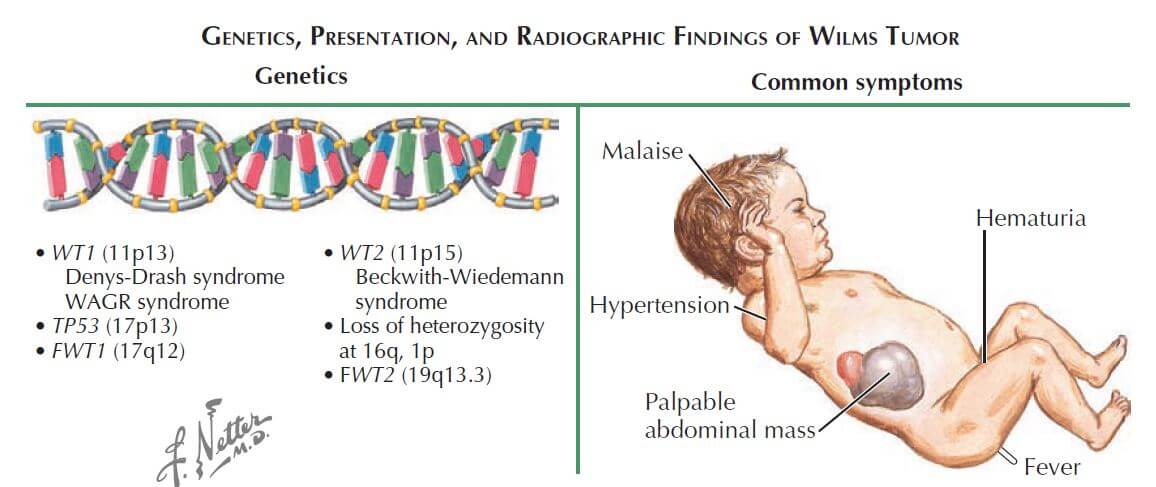
Mechanism: Deletion of WT-1 gene on chromosome 11
Pathology:
a. Macroscopic (Gross): large, solitary tan to grey color mass; pale on cut section with areas of hemorrhage; 10% are bilateral or multicentric; grossly difficult to distinguish from neuroblastoma
b. Microscopic: tumor containing 3 elements –
- Metanephric blastema
- Epithelial elements (Immature glomeruli and tubule)
- Stroma
Incidence: 1 per 10,000 children before the age of 15 years
Average age at diagnosis: 3-4 years
Symptoms:
- Usually asymptomatic abdominal mass (classic history – found during dressing or bathing)
- 20% patients present with minimal blunt trauma to mass
- Other: abdominal mass, gross hematuria, fever
Signs:
- Abdominal mass (mostly donot cross the midline)
- Hematuria (10-15%; indicates invasion of collecting system)
- Hypertension (20%; related to compression of juxtaglomerular apparatus)
- Signs of Beckwith-Wiedemann syndrome may be present
Associated syndromes:
Approx. 10% of Wilms tumors occur in children with syndromes.
1. WAGR syndrome (deletion of WT1 gene)
- Wilms tumor
- Aniridia
- Genitourinary (GU) anomalies
- Intellectual disability (mental Retardation)
2. Beckwith-Wiedemann syndrome (mutations of WT2 gene)
Others: Denys-Drash syndrome (WT1), Fraiser syndrome (WT1), Neurofibromatosis
Best initial test: Ultrasonography of abdomen
Diagnostic radiological tests: Abdominal and chest CT –
- Staging purpose
- Preoperative assessment
- Look at the contralateral kidney
Staging:
- Stage I: Limited to kidney and completely resected
- Stage II: Extends beyond kidney but completely resected; capsule invasion and perirenal tissue may be involved
- Stage III: Residual non-hematogenous tumor after resection
- Stage IV: Hematogenous metastases (lung, distal lymph nodes and brain)
- Stage V: Bilateral renal involvement
Best indicators of survival:
- Stage
- Histologic subtype: 85% have Favorable Histology (FH) with overall survival of 85% for all stages; 15% have Unfavorable Histology (UH)
Treatment:
Radical resection of affected kidney followed by:
- Lower grade tumors (I and II): Chemotherapy (Actinomycin D, i.e. DACT and Vincristine)
- Higher grade tumors (III and above): Radiotherapy
Routine pre-operative biopsy should be avoided as this upstages the tumor, requiring the intensification of chemotherapy and abdominal irradiation.
Neoadjuvant chemotherapy/radiotherapy may be required to regress the size of tumor before surgery.
This is a quick review of Wilm’s tumor on request of final year MBBS student Jaymala Shelke. For detailed information on Wilm’s tumor, refer to the textbooks.