
Before proceeding into the disease itself, let’s review – relevant anatomy of the medulla with a simple mnemonic.
The Side (lateral) part of Medulla contains 6 “S“
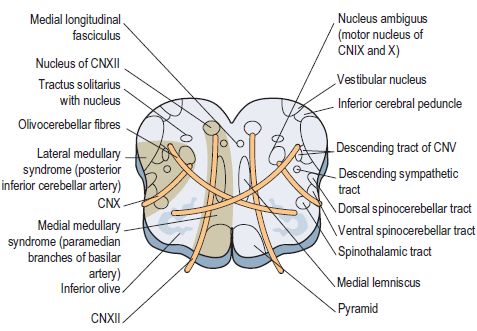
1. Spinocerebellar tract
- Posterior spinocerebellar tract: Ascends and enters to ipsilateral cerebellum via ipsilateral inferior cerebellar peduncle
- Anterior spinocerebellar tract: Ascends and enters to ipsilateral cerebellum via superior cerebellar peduncle (although it crosses to opposite side on spinal cord along with antero-lateral system, it crosses back to the same side in cerebellum)
- Cerebellar zone involved is vermis and intermediate zone (paleocerebellum) and deep nuclei involved are the medial 3 nuclei (emboliform, globose and fasciculus)
- In contrast to static proprioceptive information carried by posterior column, spinocerebellar tract carry dynamic (motion-related) proprioceptive information.
2. Spinothalamic tract (Anterolateral system)
- Crosses to opposite side of spinal cord near thier level of entry (ascends or descends 2-4 levels within the posterolateral fasciculus as they enter) and ascends to enter contralateral Ventro-posterior nucleus (VPL) thalamus directly or indirectly
- Carries information of pain, temperature and crude/light touch from the body except face
- Lateral spinothalamic tract: Pain and temperature
- Anterior spinothalamic tract: Crude touch
3. Sensory/Spinal nucleus of trigeminal nerve (CN V)
- Receives afferent from the ipsilateral face and crosses midline to enter opposite ventro-medial nucleus (VML) of thalamaus via ventral trigemino-thalamic pathway
- Although, the efferent fibers cross midline, since the nucleus is damaged in medullary lesion (and not the trigeminothalamic tract), ipsilateral loss of pain and temperature occurs
Note: Trigeminal nerve also has a primary sensory nucleus located in pons, which participates in both ventral and dorsal trigemino-thalamic pathway – while the ventral trigeminothalamic pathway crosses midline, dorsal trigeminothalamic pathway enters ipsilateral thalamus
4. Sympathetic pathway to the face
- Hypothalamospinal tract carries sympathetic fibers ipsilaterally from the hypothalamus to the intermediolateral cell column of the spinal cord to provide sympathetic stimulation to the face.
5. Speech and Swallowing nucleus (Nucleus ambiguus – CN IX and X)
- Nucleus ambiguus innervates the ipsilateral muscles of the soft palate, larynx, pharynx and upper esophagus
- Corticobulbar fibers from each hemisphere project to each nucleus ambiguus but the predominance of fibers come from the contralateral hemisphere.
- Hence, bulbar or lower motor neuron (nucleus and efferent) injury causes ipsilateral weakness but pseudobulbar or upper motor neuron (suparnuclear or corticobulbar) lesion causes contralateral weakness
6. Schwalbe (medial) and Spinal (inferior) vestibular nulceus (CN VIII)
- The vestibular complex helps control eye movements through the vestibulo-ocular pathway and helps maintain trunk and forelimb posture through the vestibulospinal and reticulospinal tracts
- There is differential involvement of the vestibular nuclei in these different tasks:
- medial vestibular nucleus is involved in all of the afferent and efferent pathways
- superior vestibular nucleus is involved in the vestibulo-ocular mechanism
- lateral (deiter) and inferior (spinal) vestibular nuclei are involved in the vestibulospinal functions.
- In lateral medullary lesions, medial and inferior vestibular nuclei may be involved:
- medial vestibular nuclei:
- vestibulo-ocular pathway (through median longitudinal fasciculus to the contralateral abducens nucleus and the efferent cross back midline to supply ipsilateral occumulotor and trochlear nucleus)
- vestibulo-spinal pathway (directly descend as medial vestibulospinal tracts and innervate cervical and upper thoracic motor nuclei – responsible for head and neck posture maintenance)
- inferior vestibular nuclei: vestibulo-spinal pathway (indirectly via reticulospinal tract to provide forelimb antigravity psoture additional to lateral vestibular nucleus)
- vestibulo-cerebellar pathway: medial and inferior vestibular nuclei sends and receives fibers from the ipsilateral midline cerebellum (flocculonodular lobe and uvula i.e. archicerebellum; deep nucleus invovled – fastigial nucleus)
- medial vestibular nuclei:
Note: Generally speaking, the superior and lateral vestibular nucleus lies in pons and the rest 2 lies in the medulla.
While the vestibulo-ocular and vestibulo-cerebellar system keeps the world straight (orientation), the spinocerebellar system keeps us straight upright (postural balance and stability).
Dentate nuclei (the lateral-most deep cerebellar nuclei) is invovled in ponto-cerebellar module (neocerebellum) which is responsible for goal-directed movements.
Except the anteromedial portion of medulla which is supplied by vertebral artery, rest of the medulla is supplied by Posterior Inferior Cerebellar Artery (PICA) – a branch of vertebral artery.
Now, after understanding the anatomy and physiology of the lateral medulla, it’s not difficult to understand the lateral medullary or Wallenberg or PICA synfrome.
Summary of the tracts and nuclei in lateral medulla
1. Spinocerebellar tract → Ipsilateral cerebellum (Anterior tract double-crosses to return back)
2. Spinothalamic tact → Contralateral VPL nucleus of thalamus (Crosses midline near the entry)
3. Spinal nucleus of trigeminal nerve → Receives afferent for pain and temperature sensation from ipsilateral face (and sends efferent to contralateral VPM nulceus of thalamus)
4. Sympathetic pathway of face → Ipsilaterally from hypothalamus to Intermediolateral cells of spinal cord gray mater
5. Schwalbe and Spinal vestibular nucleus → Vestibulo-ocular, Vestibulo-spinal and Vestibulo-cerebellar pathway
6. Speech and Swallowing nucleus → Ipsilateral innervation into muscles of soft palate, pharynx, larynx and upper esophagus (receives contralateral corticobulbar fibers)
Clinical Features of Lateral Medullary Syndrome
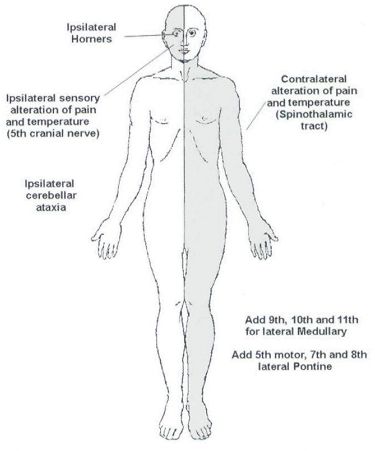
1. Spinocerebellar tract damage: Ipsilateral cerebellar ataxia
Cerebellar ataxia mnemonics:
Midline cerebellar lesion (Imbalance) – 4 T’s
- Truncal ataxia – unable to sit on bed without steadying themselves
- Titubation – bobbing motion of head or trunk
- Tandem gait positive or Rhomberg (with both eyes open and closed) positive
- Tremulous eyeballs (nystagmus)
Hemispherical cerebellar lesion (Inco-ordination) – THIRDy’s (sounds similar to 3 Dy’s)
- Tone – Hypotonic and often with pendular jerk
- Intention tremor – Coarse tremor (<5 Hz) which increases as the endpoint of intentional action
- Rebound phenomenon – Wrist when pushed quickly downward on an outstretched hand may fly back beyond original position
- Dysarthria – Scanning or staccato speech
- Dysmetria – Finger to nose or Heel to knee inco-ordination
- Dysdiadochokinesia – Irregular performance of rapid alternating movements
2. Spinothalamic tract damage: Contralateral loss of pain, temperature and crude touch from upper and lower limbs and trunks
3. Spinal nucleus of trigeminal nerve damage: Ipsilateral loss of pain and temperature sensation
4. Sympathetic pathway of face: Ipsilateral horner’s syndrome
Horner’s syndrome mnemonics: PAMELa
- Partial ptosis (loss of sympathetic supply to Muller’s muscle)
- Anhidrosis (loss of afferent to superior cervical ganglion leading to loss of hemifacial sweating)
- Miosis (loss of sympathetic supply to Dilator muscles of iris leading to unopposed cholinergic action of occumulomotor nerve)
- Enophthalmos (this is apparent rather than true enophthalmos due to narrowing of palpebral fissure)
- Loss of Ciliospinal reflex
5. Swallowing and speech nucleus (ambiguus) damage: Uvular deviation away from the side of lesion, Ipsilateral impaired palatal elevation, Dysarthria, Dysphagia and Hoarseness
6. Schwalbe and Spinal vestibular nucleus damage: Vertigo, Nystagmus, Nausea and vomiting
Cause and Mechanism of Lateral Medullary Syndrome
Posterior Inferior Cerebellar Artery (PICA) territory infarction or Vertebral artery insufficiency leading to dysfunction of multiple nuclei and damage of ascending and descending tracts on the lateral medulla.