
CAVE deformities

| Mnemonic | Deformity | Site | Components |
| C | Cavus | Midfoot | Plantar flexed 1st metatarsal |
| A | Adductus | Forefoot (Tarsometatarsal joint) | Medial displacement of navicular and cuboid along with talar neck and head; Calcaneus and distal calcaneal articulating surfaces adducted along |
| V | Varus | Hindfoot (Subtalar joint) | Calcaneum is adducted, plantar flexed and inverted along with talus |
| E | Equinus | Hindfoot (Ankle joint) | Tibiotalar and Talocalcaneal plantarflexion |
Pathoanatomy

Soft tissue shortening: On posteromedial and plantar side –
| Medial | Posterior | Plantar | |
| Muscles | TP | Tendoachilles | Abductor hallucis |
| FDL | Intrinsic flexors | ||
| FHL | Quadratus plantae | ||
| Ligaments | Deltoid | Talofibular | Plantar aponeurosis |
| Spring | Calcaneofibular | Plantar ligament | |
| Talonavicular | |||
| Capsule | Subtalar | Ankle | |
| Naviculo-cuneiform | Subtalar | ||
| Cueniform-1st MT |
Bony changes:
- Talar head and neck rotates downward and medially while the body rotates externally (reduction of normal talar body-neck angle of 160° to around 120°)
- Interosseous talocalcaneal ligament acts as the fulcrum and the anterior part of talus shifts medially and plantar wards while the posterior part of calcaneum shifts laterally and upwards (held close to fibula by calcaneofibular ligament)
- Navicular and forefoot are shifted medially and into supination along with talus
Classification
Etiologic:
- Idiopathic
- Secondary:
- Neuropathic
- Syndromic
Treatment history:
- Non-ponseti CTEV treatment: Complex clubfoot
- Ponseti CTEV treatment:
- Not Corrected: Resistant clubfoot
- Corrected: Treated clubfoot
- Deformity recurs: Recurrent clubfoot
- No treatment:
- <2 year age: Untreated clubfoot
- >2 year age: Neglected clubfoot
Pirani score and Dimeglio Classification
In metatarsus adductus, there’s only midfoot contracture score but no hindfoot contracture score during Pirani score assessment.
X-rays
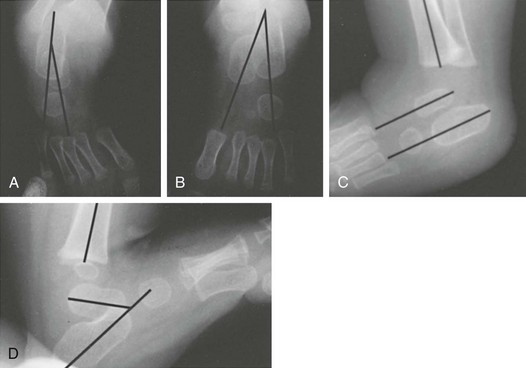
| View | Measurements | Normal | In CTEV |
| AP or Dorsoplantar (Kite’s view): Foot 30° plantarflexed and tube angled 30° in sagittal plane | Talo-1st metatarsal angle (Meary’s angle) | 5-15° | Negative (forefoot adduction) |
| Talocalcaneal (Kite’s) angle (line parallel to medial border of talus and line parallel to lateral border of calcaneus) | 30-55° | <20° (indicates varus) | |
| Lateral dorsiflexion stress (Turco’s view) | Talocalcaneal | 25-50° | <20° (indicates rocker-bottom foot i.e., failure of calcaneum to dorsiflex; dorsiflexion occurs by break in midfoot) |
| Tibiocalcaneal | 10-40° | Negative (equinus of calcaneus in relation to tibia) |
In older children, AP and lateral standing radiographs can be obtained.
Management
In order for the body of the calcaneus to evert, the anterior process of the calcaneus must first abduct. Abduction of the anterior process of the calcaneus is accomplished by abducting the forefoot as a single unit about the rearfoot by applying counterpressure against the lateral aspect of the talar head. This tri-plane maneuver initiated by the transverse plane abduction allows the heel to freely move under the talus into a more everted position with the anterior process of the calcaneus in a more abducted and dorsiflexed position.
Manipulation and serial casting (Ponseti technique)
- Treatment phase:
- Start as early as possible (possibly within 1st week of birth)
- Weekly serial manipulation and casting: Generally, 5-6 casts required (Sequence of correction is CAVE)
- Sequence of correction: CAVE
- Apply a short leg (below knee) cast and then extend to long leg (above knee) cast to:
- Maintain strong external rotation force of foot beneath the talus
- Allow stretching of medial structures
- Prevent cast slippage
- 1st cast: Correction of cavus (Elevation of 1st metatarsal and supination of forefoot; apparently deformity looks to be increased)
- Subsequent casts:
- With thumb on talar head, whole foot is abducted under talus (navicular moves away from medial malleolus and covers talar head)
- Correction of equinus:
- Do not dorsiflex until 60-70° abduction reached, talar head is covered and heel is in valgus (premature attempt to dorsiflex before correcting hindfoot varus leads to rocker-bottom foot)
- Flat-top talus (Complication of clubfoot itself vs over-dorsiflexion or cast treatment >3 months)
- Percutaneous achilles tenotomy is required in 90% cases (Pirani MFCS must be 1 or less; Talar head must be covered i.e. score for lateral head of talus is 0; heel must be in valgus and foot in abduction)
- Post-tenotomy cast for 3 weeks
- Maintenance phase: Without proper bracing recurrence occurs in 90% cases; Foot abduction orthosis (e.g.: Dennis Brown splint) – 60/30/15/1
- 60-70° External rotation (on involved side); 30-40° on normal side
- 15° Dorsiflexion
- 1 inch additional or exact width of shoulder for length of curved bar
- Full time splinting (23 hrs/day) for 3 months
- Night time splinting (12 hrs at night and 2-4 hrs at day) then upto 3-4 years age
- During day time for walking age: CTEV shoes is used
- No heel
- Straight medial border
- Lateral sole wedge
- During day time for walking age: CTEV shoes is used
- Review: 1st at 3 weeks; then 5 weekly till 1 year age; then 3 monthly till 1.5 year age; then 6 monthly till 4 years age (80% relapse in non-compliant compared to 6% in compliant patients)

Details about Ponseti technique: Clubfoot-Ponseti-Management-Red-Book-V3.pdf (steps.org.za)
Other methods:
1. Kite’s method: Cavus not addressed; Kite’s error (cuboid as fulcrum to abduct foot); Lengthy (sequential correction)
2. French method: Progressive passive manipulations, active muscle work, taping and splinting (no casting)
Atypical or complex clubfoot: Rigid equinus, Severe plantar flexion of all metatarsals, a deep crease above the heel, a transverse crease in the sole of foot, and a short and hyperextended 1st toe
– Exceptionally tight achilles tendon fibrotic upto the calf
– Forefoot will not correct upto 70° abduction but only upto 30° (which is sufficient)
– Cavus is corrected bt elevation of both medial and lateral rays (not just the 1st ray)
– Achilles tenotomy is required in all cases
Surgical treatment
Indications: 4 R
- Resistant clubfoot
- Relapsed or Recurrent clubfoot
- Remain untreated (neglected)
- Residual forefoot deformity
Timing: atleast 9-10 months when anatomy of foot can be recognized
<4 year: Soft tissue release
- Predominant equinus persisting: Posterior release
- All components of deformity persisting: Turco’s posteromedial release/PMR (Z lengthening of posteromedial muscles/tendons + Release of ligaments and capsules)
- Preserved: Anterior 1/3rd of deltoid ligament and Talocalcaneal ligament (to prevent over-correction)
- Protect: Posterior tibial artery (D.pedis artery often insufficient)
- All components of deformity persisting and rigid: Modified Mac-Kay procedure
- Complete subtalar release (Combined posteromedial and posterolateral release)
- Approach: Cincinnati approach (transverse circumferential incision)
4-10 year: Bony + soft tissue procedure
| Residual/Recurrent deformity | Surgery |
| Dynamic supination (foot supination only during walking) | SPLATT (Split anterior tibialis transfer) after 3-4 years (ossific nucleus of lateral cuneiform appears) |
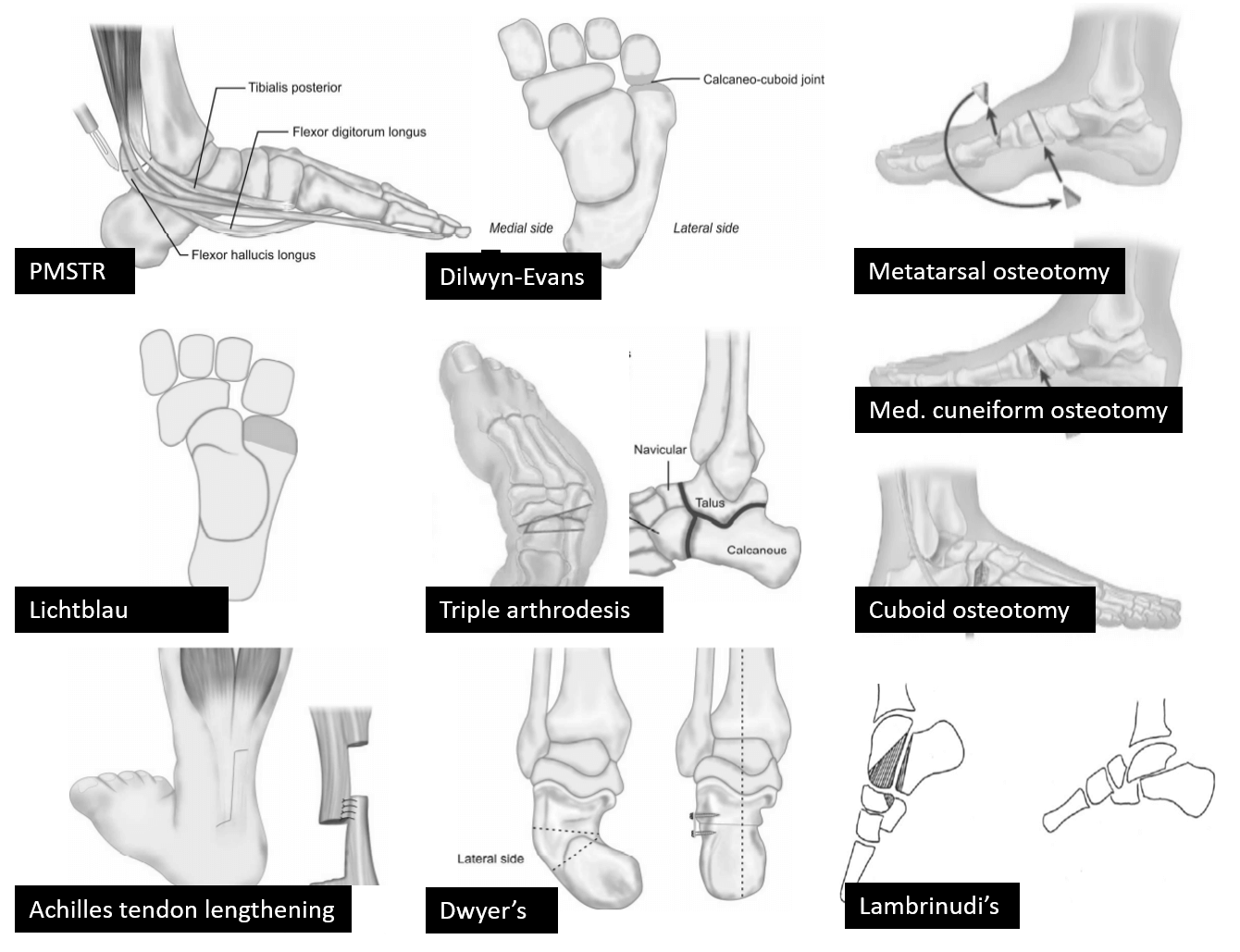
| Rigid forefoot adduction or supination or both | Double tarsal wedge osteotomy: Medial cuneiform (open wedge) and cuboid (close wedge) osteotomies in >6 years |
| Isolated heel varus | Dwyer’s osteotomy (medial open wedge osteotomy of calcaneus) Modification (lateral close wedge osteotomy of calcaneus) |
| Heel varus with residual internal rotation of calcaneus with a long lateral foot column | Lichtblau’s procedure (lateral close wedge osteotomy of anterior end of calcaneus) |
| Midfoot varus due to talonavicular and calcaneo-cuboid subluxation | Dilwyn-Evan’s procedure (PMR + Calcaneo-cuboid wedge resection and arthrodesis) |
| Internal rotation of foot | Supramalleolar osteotomy |
| Metatarsus adductus | Metatarsal osteotomy |
| Equinus | Achilles tendon lengthening + Posterior capsulotomy of subtalar and ankle joint |
| Severe, rigid, recurrent clubfoot in arthrogryposis | Talectomy |
>10-12 year:
- All three deformities of hindfoot varus: Triple arthrodesis (correction by lateral closing wedge osteotomy through subtalar and midtarsal joints)
- Rigid equinus: Lambrinudi arthrodesis (distal-plantar bone wedge removed from talus and triangular beak of talus is wedged into notch created in navicular and subtalar joint followed by triple arthrodesis)
- Gradual distraction and correction in External fixator


He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music.