
Heart Tube
At the beginning of 4th week of development, heart is a continuous and valveless linear tube that resembles a chicken hung upside-down. It consists of 5 embryonic dilatation, that are destined to be the inflow and outflow tract and compartments of the hear without septum and valves.
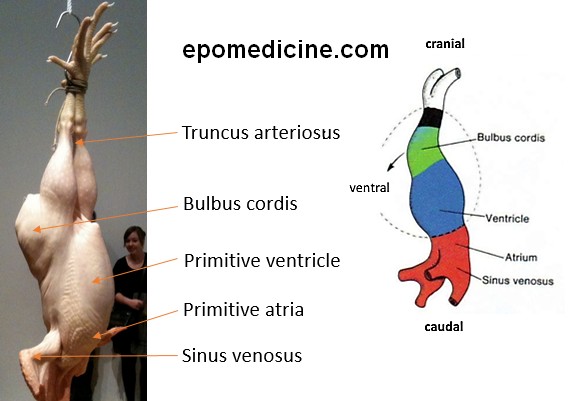
1. Legs: Outflow (truncus arteriosus); 2. Wings: Inflow (Sinus venosus); 3. Thigh: Bulbus cordis; 4. Breast: Primitive ventricle and primitive atria
From cranial to caudal, these dilations are:
- Truncus arteriosus (arteries)
- Ascending aorta
- Pulmonary trunk
- Distal end dilates to form aortic sac which divides into right and left limbs. Each limb is connected to corresponding dorsal aorta through 6 aortic arches.
- Bulbus cordis
- Smooth part of left (conus arterious) antd right ventricles (aortic vestibule)
- Primitive ventricle
- Trabeculated part of left and right ventricles
- Primitive atrium
- Trabeculated part of left and right atrium
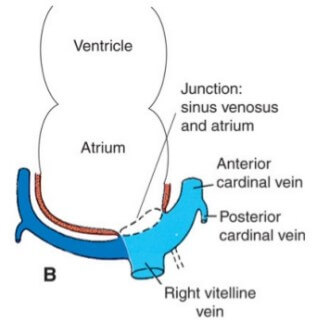
- Sinus venosus
- Right – smooth part of right atrium (sinus venarum)
- Left – coronary sinus
- Oblique vein of left atrium
Smooth part of left atrium is formed by primitive pulmonary veins.
Crista terminalis: Junction of the trabeculated and smooth parts of the right atrium
Dextral looping
- The heart tube grows and starts to bend to the right at day 22 and is completed by the end of 4th week (day 28)
- Retinoic acid is thought to act as a signal for antero-posterior values in heart development.
- Looping depends on the laterality inducing genes.
- Looping aligns the future atria, ventricles, inflow and outflow tract.
- During this process, the proepicardial cells invest the outer layer of heart tube and eventually form epicardium and coronary vasculature.
- Here, we will use the analogy of inverted sit ups to imagine how the looping occurs and how it positions the embryonic dilations of heart tube.
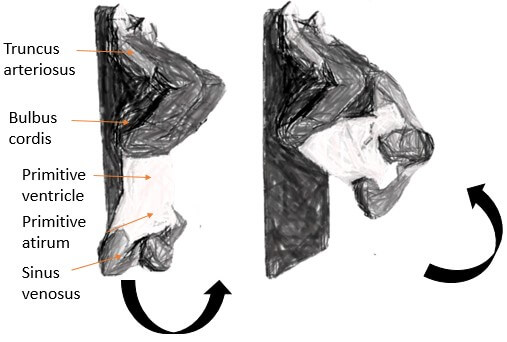
Ventricle goes to the left.
Atrium moves posteriorly and superiorly.
As the heart continues to grow and bend – bulbus and ventricles come to lie side by side and ventral to atrium.
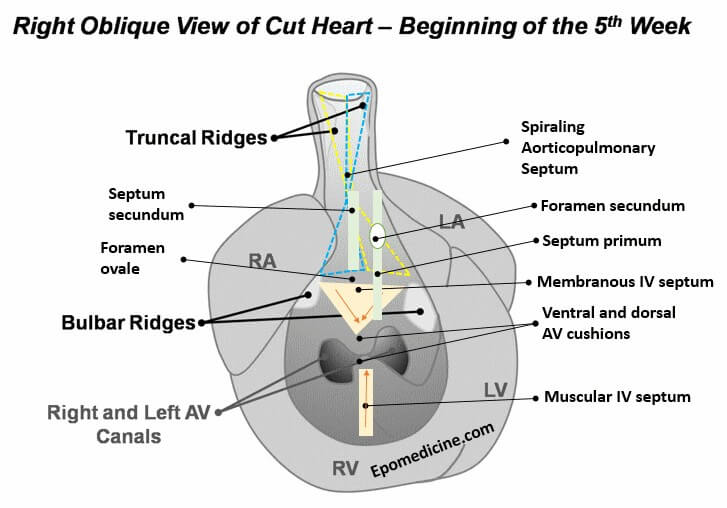
1. AP septum: Neural crest cells invade truncal and bulbar ridges leading to their growth in spiral fashion and formation of AP septum
2. Interatrial septum: Septum primum grows towards AV cushion and closes foramen primum but has foramen secundum in center. Septum secundum grows to the right and the gap between its upper and lower limb is foramen ovale.
3. AV septum: Ventral and dorsal AV cushion fuses to form right and left AV canal.
4. Interventricular spetum: Muscular IV septum grows from the floor of ventricle towards AV cushion and remaining gap is IV foramen. Membranous IV septum is formed by fusion of both bulbar ridges with dorsal AV cushion to close IV foramen.
Timeline of Other Important Events
| Normal Time | Developmental Events | Malformations arising during period |
| Mid 3rd week | Horseshoe-shaped cardiac primordium appears.
2 Endocardial tubes form on either side of neural plate.
|
Lethal mutations |
| 20 days | Bilateral Endocardial tubes fuse to form a single heart tube.
|
Cardiac bifida (experimental) |
Cardiac jelly appears.
|
||
Aortic arch is forming.
|
||
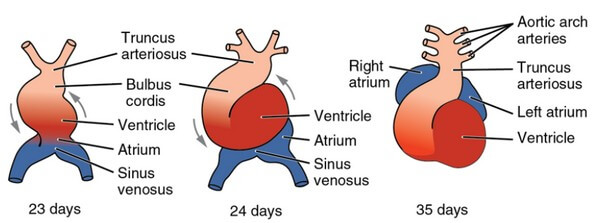
| 22 days | Heart is looping into S shape. | Dextrocardia
|
| Heart begins to beat. | ||
Dorsal mesocardium is breaking down.
|
||
| Aortic arches I and II are forming. | ||
| 24 days | Atria are beginning to bulge. | |
| Right and left ventricles are likely to pump in series. | ||
| Outflow tract is distinguished from right ventricle. | ||
| Late week 4 | Sinus venosus is being incorporated into right atrium. Sinus venosus receives 3 sets of veins on either horns:
|
Venous inflow malformations |
Endocardial cushions appear. Endocardial cushions are derived from:
Once, EMT has occured, both types of cells proliferate and invade the Cardiac Jelly, to form the endocardial cushions. Sox9 plays an important role in endocardial cushion formation. |
Persistent common atrioventricular canal
|
|
| Septum primum appears from primitive atrial roof between right and left atria. | Common atrium (Cor triloculare biventriculare):
|
|
Muscular interventricular septum is forming from the floor of primitive ventricle.
|
Common ventricle | |
Truncoconal ridges are forming.
|
Persistent trucus arteriosus
|
|
| Aortic arch I is regressing. | ||
| Aortic arch III is forming. | ||
| Aortic arch IV is forming. | ||
| Early week 5 | Endocardial cushions are coming together, forming right and left atrioventricular canals. | Persistent atrioventricular canal. |
Sinoatrial orifice shifts to right:
|
||
| Further growth of interatrial septum primum and muscular interventricular septum occurs. | Muscular ventricular septal defects | |
Truncus arteriosus is dividing into aorta and pulmonary artery.
|
Transposition of great vessels:
Tetralogy of Fallot:
|
|
| Atrioventricular bundle is forming; there is possible neurogenic control of heartbeat. | ||
Pulmonary veins are being incorporated into the left atrium.
|
Aberrant pulmonary drainage | |
Aortic arches I and II have regressed.
|
||
Aortic arches III and IV have formed.
|
||
Aortic arch VI is forming.
|
||
| Late week 5 to Early week 6 | Endocardial cushions fuse.
|
Persistent common AV canal:
|
| Interatrial foramen secundum is forming in septum primum. | ||
| Interatrial septum primum is almost contacting endocardial cushions (for closure of foramen primum). | Low atrial septal defects | |
Membranous part of interventricular septum starts to form.
|
Membranous ventricular septal defect
|
|
Semilunar valves begin to form.
|
Aortic and pulmonary vascular stenosis | |
| Late week 6 | Interatrial foramen secundum is large. | High atrial septal defects |
Interatrial septum secundum starts to form.
|
Foramen secundum defect: Excessive resorption of septum primum or secundum or both. It may be tolerated for a long time. | |
| Atrioventricular valves and papillary muscles are forming. | Ebstein’s anomaly:
Tricuspid atresia (hypoplastic right heart):
|
|
| Interventricular septum is almost complete. | Membranous ventricular septal defects | |
| Coronary circulation is being established. | ||
| 8-9 weeks | Membranous part of interventricular septum is complete.
|
Membranous ventricular septal defects |


He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music.