
Synonyms: Extensor expansion, Extensor hood, Dorsal expansion, Dorsal hood, Dorsal aponeurosis
Components:
- Extrinsic tendons
- Intrinsic tendons
- Soft-tissue stabilizing structures

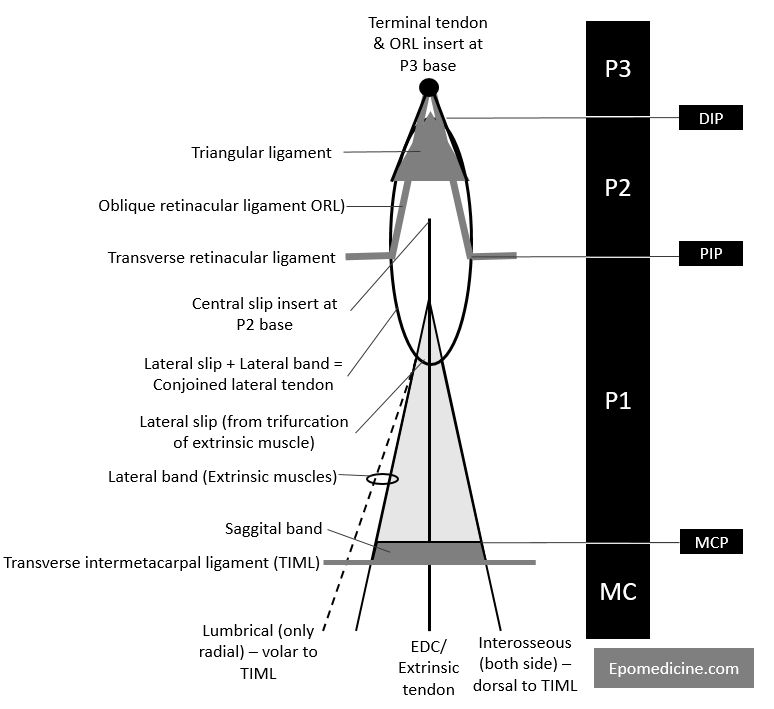
MC (metacarpal); P1 (proximal phalanx); P2 (middle phalanx); P3 (distal phalanx)
Extrinsic tendon
Extensor Digitorum Communis (EDC; may be absent in little fingers) ± Extensor Indicis Proprius (EIP; usually ulnar to EDC) ± Extensor Digiti Minimi (EDM; ulnar to EDC) passes dorsally over MCP joint and trifurcates:
- Central slip: Inserts into dorsal middle phalanx base (rupture leads to boutonniere deformity)
- 2 Lateral slips: Join with the lateral bands formed by intrinsic muscles (Interosseous ± Lumbrical) to form conjoined lateral band.
Intrinsic tendon
- Interosseous: Travel dorsal to transverse intermetacarpal ligament on both sides
- Lumbrical: Travels volar to transverse intermetacarpal ligament only on radial side
Both the intrinsic muscles travel volar to the metacarpophalangeal joint’s axis of rotation – hence, they aid in MCP flexion.
Interosseous slip ± Lumbrical (radial) slip = Lateral band
Lateral band + Lateral slip of EDC = Conjoined lateral band
2 Conjoined lateral bands converge at dorsal distal phalanx base = Terminal extensor tendon
MCP joint control:
- If this joint is fully extended, the interossei extend the last two phalanges (middle and distal phalanx) through the lateral bands.
- If the MCP is flexed to 90 degrees, the interossei only strengthen the flexion of the proximal phalanx.
- If the MCP joint is in the intermediary position, the interosseous ligaments have a dual function: stabilization of the MCP joint and extension of the distal phalanges.
Lumbricals: contribute to extension of the PIP and DIP joints by –
- Opposing the pull from the FDP through their direct insertion on it
- Synergy with the common extensor
Soft-tissue stabilizing structures
- Sagittal bands: Connect the extrinsic tendon to MCP joint volar plate and deep transverse metacarpal ligament
- Primary stabilizer of extensor tendon at MCP joint
- Transverse retinacular ligament: Connect the lateral bands to PIP joint volar plate
- Attenuation = Dorsal translation of lateral bands = PIPJ hyperextension = swan-neck deformity
- Contracture = Volar translation of lateral bands = PIPJ flexion = boutonniere deformity
- Triangular ligament (Triangle of stack): Counteracts transverse and oblique retinacular ligament to prevent volar subluxation of lateral bands
- Oblique retinacular ligament (ORL): variably present and assist with linking IP joint motion
- Arises from volar plate of PIP joint and flexor tendon sheath and insert onto dorsal base of distal phalanx
- PIP flexion relaxes ORL allowing DIP flexion and PIP extension tenses ORL extending the DIP
- Retraction leads to boutonnière deformity of finger
Proximal phalanx is controlled by: Extensor, Flexors and Interossei
Middle and distal phalanx is controlled by: Extensor, Flexors and Retinacular ligaments
Extensor apparatus of thumb: It is less complex and comprises of –
a. Extrinsic tendons: EPL (to dorsal base of distal phalanx) and EPB (radial to EPL and inserts on dorsal base of proximal phalanx)
b. Intrinsic tendons: APB and FPB
c. Soft-tissue stabilizing structures: 2 saggital bands (connect EPL to MCP volar plate)
Few mnemonics that may be handy:
- eXtensor eXpansion is in proXimal phalanX
- Lumbrical is a part of Lateral band only Laterally (radial side)
- Central slip of Common extensor tendon (Communis) inserts into Central (middle) phalanx
- Lateral band inserts into Last (distal) phalanx
References:
1. ASSH Manual of Hand Surgery edited by Warren C. Hammert, David J. Bozentka, Martin I. Boyer
2. Musculoskeletal key – Injuries of the Extensor Apparatus
Try yourself and Answer (in comments)
- We can extend the PIP and DIP joint without extending the MCP joints. But we can’t extend the PIP joint without extending the DIP joint at the same time. Why?
- Flexing only the DIP joint without concurrently flexing PIP joint is difficult. Why?
- Full flexion of PIP joint prevents active extension of DIP joint. Why?