
4 week embryo
5 mesenchymal prominences (facial primordia) appear in relation to the stomodeum (a depression in the surface ectoderm which marks the future mouth and oral cavity):
- Cranially: Frontonasal prominence (unpaired)
- Laterally: Maxillary prominence (paired; 1st pharyngeal arch)
- Caudally: Mandibular prominence (paired; 1st pharyngeal arch)
5 week embryo
Localized surface ectodermal thickening gives rise to sensory placodes:
- Nasal placode: forms olfactory epithelium
- Lens placode: forms lens
Nasal placode sinks into the underlying mesenchyme to form 2 blind-ended nasal pits (primitive nasal cavity).
Proliferation of mesenchyme from frontonasal process around the opening of nasal pits form: medial and lateral nasal prominences.
Nasal pits continue to deepen until they:
- Enlarge and fuse to form single ectodermal nasal sac.
- Approach the roof of primitive oral cavity, being partitioned from it by oronasal membrane.
By the end of 5th week – oronasal membrane ruptures into posterior choana establishing communication between oral and nasal cavities.
6 week embryo
The prominences begin to fuse with eachother.
- 2 mandibular prominences fuse in the midline: Tissues of lower jaw and lower lips
- Mandibular prominence and maxillary prominence: At angle of mouth
- Lateral nasal prominence and maxillary prominence: Forms ala of nose
- 2 Medial nasal prominences fuse in midline to form intermaxillary segment:
- Labial component: philtrum of upper lip
- Upper jaw component: which carries 4 incisor teeth
- Primary palate (hard palate anterior to incisive foramen)
- Primary nasal septum also forms from frontonasal process
- Medial nasal prominence and maxillary prominence:
- Lateral portion of upper lip
- Lateral portion of maxilla
Naso-optic furrow develops (between merging lateral nasal prominence and maxillary prominence): Epithelial cord sinks in the mesenchyme –
- Lower part: Canalizes to form nasolacrimal duct
- Upper part: Expands to form lacrimal sac
Labiogingival laminae (ectodermal ingrowth) along the edge of upper jaw:
- Forms upper lip and alveolus
- Degenerates leaving labioginigval groove: Only frenulum remains between lips and gingiva
2 lateral palatal shelves develop from maxillary processes behind the primary palate.
By the end of 6th week:
- Primitive nasal cavities are separated by a primary nasal septum.
- Primitive nasal cavities are partitioned from oral cavity by primary palate with larger oronasal cavity behind.
- Secondary nasal septum develops from stomodeum behind the primary nasal septum – dividing the nasal part of oronasal cavity.
- 2 lateral palatal shelves have developed behind primary palate.
7 week embryo
Oral part of oronasal cavity becomes completely filled by the developing tongue.
8 week embryo
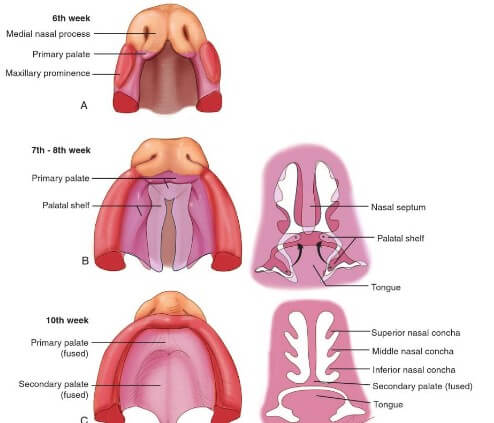
Palatal shelves merges with each other and secondary nasal septum in the midline to form definitive or secondary palate.
Secondary palate (posterior to incisive foramen) makes contact with the primary palate (anterior to incisive foramen) to completely divide oral and nasal cavities.
12 week embryo
Fusion of palatal shelves (palatine processes), primary palate and secondary nasal septum is complete.
Fusion of processes on the face completes.
12-16 week embryo
Invasion of anterior palate by bone and posterior palate by muscle of 1st and 4th pharyngeal arches to form bony palate and soft palate.
Facial clefts
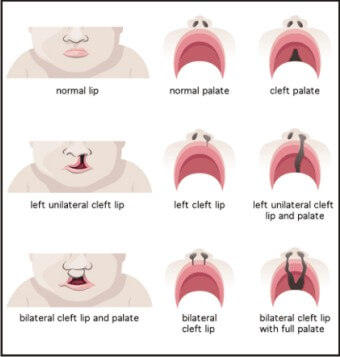
Failure of the embryonic facial prominences to fuse properly –
Median cleft lip: failure of medial nasal prominences to fuse and form intermaxillary segment.
Unilateral cleft lip: results from failure of the maxillary prominence to merge with the medial nasal prominence on the affected side
Bilateral cleft lip (Hare lip): results due to failure of maxillary prominences to meet and unite with the medial nasal prominences on both sides
Oblique facial cleft: results from failure of the maxillary prominence to fuse with the lateral nasal prominence.
Macrostoma: incomplete lateral fusion of maxillary and mandibular prominences.
Anterior cleft palate (anterior to incisive foramen): palatine shelves fail to fuse with primary palate
Posterior cleft palate (posterior to incisive foramen): palatine shelves fail to fuse with each other and secondary nasal septum
Anteroposterior cleft palate: Combination of both the anterior and posterior defects