
Endpoints of resuscitation
MAP: > or = 65 mmHg
Urine output: > 0.5 ml/kg/hr; despite ↓RBF (Renal Blood Flow) it can be normal due to –
- Atrial natriuretic factor are elevated in sepsis
- Hypoproteinemia in sepsis – low plasma colloid osmotic pressure is less able to facilitate oncotic reabsorption.
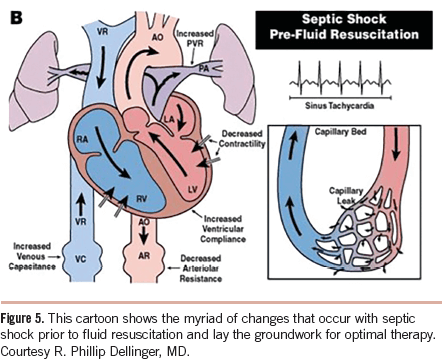
CVP: 8-12 mmHg; may be unreliable due to –
- decreased ventricular compliance, increased airway pressure from ventilation, tricuspid regurgitation, pulmonary hypertension, and ventilation/perfusion abnormalities in the lung
Oxygen delivery and oxygen consumption: SvO2 > or = 65%
- Oxygen delivery (mL/min) = CO (L/min) X Hb concn. (g/dL) X 1.34 (mL O2/g Hb) X % SaO2
- Oxygen consumption = CO X (SaO2-SvO2) X 1.34 (Hb concn.)
- An SvO2 less than 50% is highly suggestive of decreased perfusion
- SvO2 may be high in sepsis due to increased blood flow to metabolically inactive tissue
Lactate/base excess: Serial ABG measurements (>4 mmol/l ~ severe sepsis)
- Increased glycolysis (increased pyruvate) with inhibition of pyruvate dehydrogenase (by endotoxin)
Echocardiography and Doppler:
- Changes in aortic blood flow velocity with respiration (accurate if systolic function is preserved)
Pulse pressure variability with respiration:
- As patients become more hypovolemic, pulse pressure variability increases.
Sepsis Bundle as per Surviving Sepsis Campaign
TO BE COMPLETED WITHIN 3 HOURS OF TIME OF PRESENTATION:
1. Measure lactate level
2. Obtain blood cultures prior to administration of antibiotics
3. Administer broad spectrum antibiotics
4. Administer 30ml/kg crystalloid for hypotension or lactate ≥4mmol/L
TO BE COMPLETED WITHIN 6 HOURS OF TIME OF PRESENTATION:
5. Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) ≥65mmHg
6. In the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was ≥4 mmol/L, re-assess volume status and tissue perfusion.
7. Re-measure lactate if initial lactate elevated. 1http://www.survivingsepsis.org/SiteCollectionDocuments/SSC_Bundle.pdf
Basic Approach to Early Goal Directed Therapy (EGDT)
- Crystalloids or colloids if CVP <8
- Vasoactive agents when CVP goals will be met but mean arterial pressure (MAP) remains <65 mm Hg
- ScVO2 of < 70% for transfusion of packed red blood cells to target hematocrit of 30% (or the use of inotropic agents if hematocrit already >30%)
Fluid Resuscitation Recommendations
- Crystalloid or colloid – Crystalloid as first choice; HES not to be used and albumin to be used when large volume of crystalloids is required
- Initial fluid challenge – atleast 30 mL/kg of crystalloids (or colloid equivalent)
- Fluid challenge continued – until hemodynamic improvement either based on:
- dynamic (eg, change in pulse pressure, stroke volume variation) or
- static (eg, arterial pressure, heart rate, CVP) variables. 2http://www.sccm.org/Documents/SSC-Guidelines.pdf
Vasopressor Recommendations

- Indicated if MAP <65 mmHg despite fluid challenge
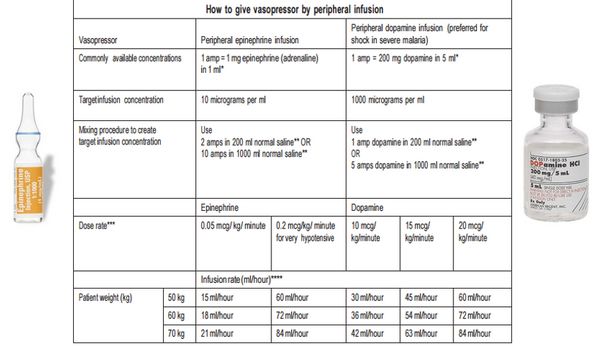
- Vasopressors may be started from peripheral line but central line must be established as soon as possible.
- 1st choice: Norepinephrine (NE)
- Start with a dose rate of 0.1 microgram/kg/min and titrate upward as needed.
- Dose rates up to 3.3 microgram/kg/min are successful in raising the blood pressure in most cases.
- If the desired MAP is not achieved at a dose rate of 3–3.5 microgram/kg/min, add a second vasopressor.
- Norepinephrine is favored by many because it is more likely to raise the blood pressure than dopamine, and is less likely to promote arrhythmias. 3Marino P. Marino’s the ICU book. 4th ed. Wolters Kluwer Health; 2014.
- Epinephrine may be added to norepinephrine or replace norepinephrine to maintaing target goals if not achieved
- Vasopressin 0.03 units/minute can be added to NE to raise MAP or decrease NE dosage.
- Doses higher than 0.03-0.04 units/minute as a salvage therapy (reserved for failure to achieve adequate MAP with other vasopressor agents)
- Vasopressin is a pure vasoconstrictor that can promote splanchnic and digital ischemia, especially at high dose rates.
- Dopamine can be used instead of norepinephrine only if patient has low cardiac risk
- Start at a dose rate of 5 microgram/kg/min and titrate up-ward as needed.
- Vasoconstriction is the predominant effect at dose rates above 10 microgram/kg/min.
- If the desired MAP is not achieved with a dose rate of 20 ∝g/kg/min, add NE as a second vasopressor.
- Reno-protective low dopamine dosing is a myth.
- Phenylephrine can be used only when:
- Serious arrhythmias associated with norepinephrine
- High cardiac output with low blood pressure persistently (phenylephrine is a potent vasoconstrictor)
- As salvage therapy when combined vasopressors have failed to achieve MAP target
Blood Products Recommendations
- Once tissue hypoperfusion has resolved and in the absence of myocardial ischemia, RBC transfusion to be carried only when hemoglobin concentration decreases to <7.0 g/dL
- Target adult hemoglobin 7.0 –9.0 g/dL
- Erythropoietin should not be used as a specific treatment of sepsis associated anemia
- Fresh frozen plasma to be used only in cases of active bleeding or planned invasive procedure in the setting of deranged clotting profiles.
- Antithrombin not to be used for the treatment of severe sepsis and septic shock