
Pre-eclampsia is a disorder of pregnancy, characterized by hypertension (BP > 140/90 mmHg measured 2 times with interval ≥ 6 hours) and proteinuria (urinary excretion of ≥ 0.3 gm protein/24 hour specimen or 1+ in dipstick) after the 20th weeks of gestation in a previously normotensive and non-proteinuric woman. Pre-eclampsia when complicated with generalized tonic clonic convulsion and/or coma is called Eclampsia. Severe pre-eclampsia is defined by a systolic BP ≥ 160 mmHg or a diastolic BP ≥ 110 mmHg twice 6 hour apart at bed rest with or without the following end-organ findings: Proteinuria of ≥5 gm in a 24-hour urine specimen (or 3+ on random urine dip on two occasions at least 4 hours apart), Oliguria (<500 mL in 24 hours), Neurologic or visual disturbances (including headache), Pulmonary edema, Elevation of transaminases, Epigastric or right upper quadrant pain, Thrombocytopenia, Fetal growth restriction or Eclampsia.
Mechanism of Action of Magnesium Sulfate/Sulphate (MgSO4):
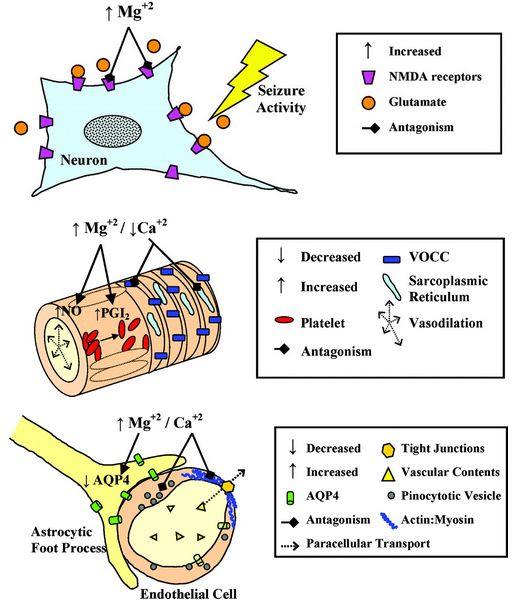
The mechanism of action of Magnesium sulfate in eclampsia is not clear. The postulated mechanisms are:
a. Central action: Voltage dependent blockade of NMDA (N-methyl D-aspartate) subtype of glutamate (excitatory) channel receptors
b. Peripheral action: At Neuromuscular Junction (NMJ), it causes –
- Blockage of calcium entering the cell and blocking calcium at intracellular sites/membranes
- Reduction of presynaptic acetylcholine (ACh) release at the endplate
- Reduction of motor endplate sensitivity to acetylcholine (ACh)
Role in Severe pre-eclampsia and Eclampsia:
Magnesium sulfate is an anticonvulsant rather than an anti-hypertensive. It prevents seizures in pre-eclampsia and doesn’t treat hypertension. In eclampsia, it is given as soon as the convulsion has ended. It causes vasodilation, increases cerebral, uterine and renal blood flow. It decreased cerebral edema.

- “x” % of Magnesium sulfate contains “x” gm in 100 ml
- 1 ampoule contains 50% of 2 ml Magnesium sulfate
- 1 ampoule contains 1 gm of Magnesium sulfate in 2 ml
- 4 ampoule provides 4 gm of Magnesium sulfate in 8 ml
- To prepare 20% of 4 gm Magnesium sulfate, “y” ml of Normal saline (NS) must be added:
- 20 gm/100 ml = 4 gm/(8 ml + “y” ml)
- 8 + “y” = 20
- “y” = 12
Pritchard Regimen:
a. Loading dose:
Initially: 4 gm of 20% MgSO4 IV over not less than 3 minutes
- Take one 20 ml syringe
- Draw 4 ampoules of Magnesium sulfate
- Add 12 ml Normal saline
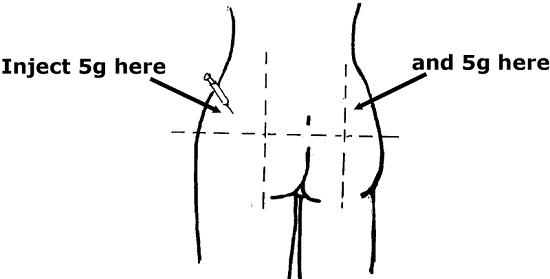
Immediately followed by: 10 gm of 50% MgSO4 IM (5 gm in each buttock)
- Take two 10 ml syringes
- Draw 5 ampoules of MgSO4 in each syringe
- Add 1 ml of 2% Lignocaine in each syringe
- Give deep IM in each buttocks
If convuslion persists after 15 minutes: 2 gm of 50% MgSO4 IV bolus over 5 minutes
- Take one 10 ml syringe
- Draw 2 ampoules of Magnesium sulfate
b. Maintenance dose:
5 gm of 50% MgSO4 IM 4 hourly in alternate buttocks
- Take one 10 ml syringe
- Draw 5 ampoules of MgSO4
- Add 1 ml of 2% Lignocaine in each syringe
- Give deep IM 4 hourly in alternate buttocks
- Continue for 24 hours after the last convulsion or delivery whichever is later.
Monitoring Hourly for Magnesium Sulfate toxicity:
Suspend or postpone use of Magnesium sulfate, if any of the following is present:
- Respiratory rate < 16/min (Respiratory depression)
- Absent patellar reflex (Muscle paresis)
- Urine output < 30 ml/hour in preceding 4 hours (Impaired renal function)
Note: Loss of patellar reflex is the 1st sign of Magnesium toxicity. The therapeutic level of serum magnesium is 4-7 mEq/l. Serum levels of Magnesium toxicity:
- 8-12 mEq/l: Loss of patellar reflex, flushing, warmth, somnolence, slurred speech
- 15-17 mEq/l: Muscular paralysis, Respiratory difficulty
- 30-35 mEq/l: Cardiac arrest
Management of Magnesium Sulfate toxicity:
a. If urine output < 30 ml/hour:
- MgSO4 withheld
- IV ringer lactate infusion 1 liter over 8 hours
- Monitor for pulmonary edema
b. If respiratory arrest occurs:
- Perform assisted ventilation
- Antidote: Calcium gluconate 1 gm (10% of 10 ml) IV slowly over 10 minutes
Contraindication of Magnesium Sulfate:
- Myasthenia gravis
- Impaired renal function
Other Magnesium Sulfate regimens:
- High dose regimens (Loading dose > 10 gm): Pritchard, Lucas
- Low dose regimens (Loading dose < 10 gm): Zuspan or Sibai, Suman sardesai
- Loading dose: 4-6 gm IV over 15-20 minutes
- Maintenance dose: 1-2 gm/hr IV infusion
- Single dose regimen: VIMS regimen
- single doses of 4g diluted 50% Mgso4 intravenously, with simultaneous 4g 50% MgSo4 intramuscularly.
Note: Researches have found that the Zuspan regimen is upto 8 times less effective than the Pritchard regimen in preventing convulsions in severe pre-eclampsia and eclampsia. The ‘VIMS’ regimen can be used at First Referral Units, before shifting the patients to tertiary care centres. This approach has special implications in the developing countries, especially at the primary care level, where the standard obstetric care is not widely available.
‘Single Dose MgSo4 Regimen’ for Eclampsia – A Safe Motherhood Initiative. – ResearchGate. Available from: http://www.researchgate.net/publication/243970655_’Single_Dose_MgSo4_Regimen’_for_Eclampsia_-_A_Safe_Motherhood_Initiative
Magnesium sulfate is preferred over Diazepam and Phenytoin because:
- Relatively less depression effect to mother or fetus
- Reduced risk of convulsions
Disclaimer: This is only for learning purpose and should not be used as a medical advice
Also Read about Bishop Scoring in Obstetrics