
Mnemonic: BURNS
Burn depth and body surface area (BSA)
| Burn degree | Burn depth | Features | Healing |
|---|---|---|---|
| Mnemonic: Number of degrees = Number of structures involved | Mnemonic: RBCS | ||
| 1st | Superficial (epidermis only) | Red | <1 wk |
| 2nd | Partial thickness – superficial (epidermis + papillary dermis) | Blister + Blanches | 1-3 wks |
| Partial thickness – deep (epidermis + reticular dermis) | Compared to superficial partial thickness: Deep = Dermal appendages involved + Decreased: a. Moistness (Dry) b. Color (Mottled red) c. Blanching d. Pain | >3 wks, usually requires surgical treatment | |
| 3rd | Full thickness (epidermis + dermis + subcutaneous fat) | Charred and Contractures (leathery dry, no blanching, painless) | Rare, unless surgical treatment |
| 4th | Epidermis + dermis + subcutaneous fat + fascia/muscle/bone | Surrounding area (second degree) pain increased | Never – requires surgical treatment |
Burned Body Surface Area (BSA) for 2nd and 3rd degree burns
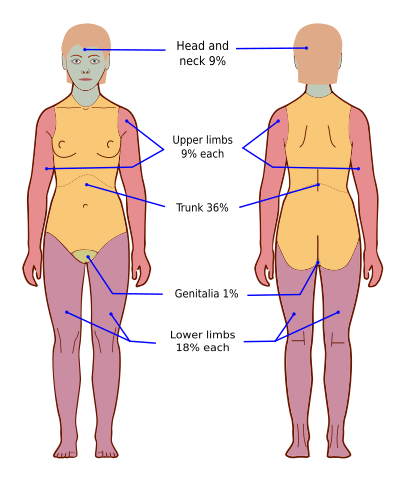
Wallace Rule of 9:
| Structures | BSA (%) – Adults | BSA (%) – Infants |
|---|---|---|
| Head and neck | 9 | 18 |
| Upper limbs (each) | 9 | 9 |
| Trunk – anterior | 18 | 18 (trunk and perineum) |
| Trunk – posterior | 18 | 18 (including 2.5% for each buttock) |
| Perineum | 1 | |
| Lower limbs (each) | 18 | 14 |
Comparison with other methods
| Lund & Browder | Rule of 9s | Palmar | |
|---|---|---|---|
| Theory | Age-based assessment | Body divided in 9% areas | Patient’s palm is 1% |
| Advantages | “Gold-standard” accuracy | Efficient | Minor Burn Estimation |
| Disadvantages | Inefficient | Over-estimation | User variability |
Mortality prediction:
3 factors: Mnemonic – BAI
- Burn BSA >40%
- Age >60 years
- Inhalational injury
Baux score (% mortality) = Age + BSA
- BSA >70% in elderly or Baux score >130 = Near 100% mortality
- Score <80 is considered good and >100 is considered bad
Revised Baux score = Baux score + 17 (for inhalational injury)
Urine output monitoring
Aim:
- Adults: 0.5 ml/kg/hr
- Children <30 kg: 1 ml/kg/hr
- Electrical injury: 1-1.5 ml/kg/hr
Resuscitation and Referral
a. Early intubation: Indications –
- Airway obstruction signs (hoarseness, stridor, retractions)
- Burn surface area >40-50%
- Circumferential neck burns
- Deep facial burns
- Edema (significant)
- Fatigue of respiration
- GCS <8
- Hypoxemia despite 100% 0xygen, Hypoventilation (PCO2 >50 mmHg and pH <7.2)
b. Fluid resuscitation: For 2nd and 3rd degree burn >20% BSA
Initial resuscitation with warmed RL
| Fluid | Adult | Pediatric (<14 year) | Electrical burn |
|---|---|---|---|
| Rate | 2 ml X kg X BSA | 3 ml X kg X BSA | 4 ml X kg X BSA |
| Children <30 kg | + 3 ml X kg X BSA D5RL at maintenance rate | RL |
If the initial resuscitation rate fails to produce the target urine output, increase the fluid rate until the urine output goal is met.
Follow 4-2-1 rule for maintenance fluid rate.
c. Referral to burn center: Indications –
- Second degree (partial thickness) burn >10% BSA
- Third degree (full thickness) burn
- Burns to face, hand, feet, genitalia or major joints
- Electrical, chemical or inhalational burns
- Comorbidities
- Concomitant trauma
- Patients requiring special social, emotional or rehabilitative intervention
- Pediatric burns without qualified personnel or equipment
NG decompression
Indications:
- Nausea/vomiting
- Abdominal distension
- Burns >20%
Surgery
Conservative management is appropriate for superficial burns and mixed superficial burns that will heal in 2 weeks. More complex burns may require excision and skin grafting. Excision and primary closure is not generally practiced as there is a high risk of infection.
Escharotomy:
- Indicated in circumferential full thickness burns to the torso or limbs.
- Careful division of the encasing band of burn tissue will potentially improve ventilation (if the burn involves the torso), or relieve compartment syndrome and oedema (where a limb is involved)
Reference: ATLS 10th edition