
Anatomy:

a. Outline of base of tongue.
b. Vallecula.
c. Hyoid bone.
d. Epiglottis and aryepiglottic folds.
e. Arytenoids.
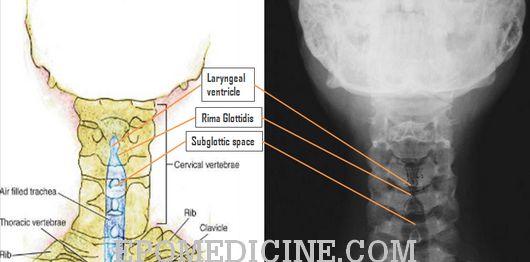
f. False and true cords with ventricle in between them.
g. Thyroid and cricoid cartilages.
h. Subglottic space and trachea.
i. Prevertebral soft tissues.
j. Cervical spine.
k. Pretracheal soft tissues and thyroid.
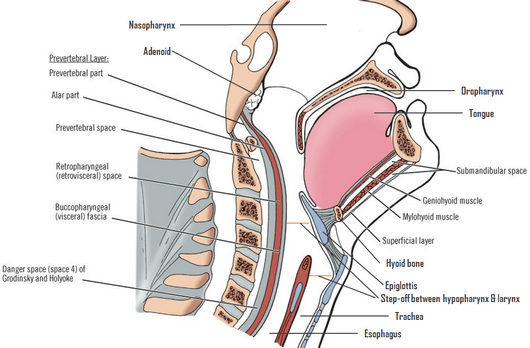
Retropharyngeal space: Extends from the base of the skull down to the level of the carina, and is located between the buccopharyngeal mucosa and the prevertebral fascia.
Prevertebral space: A potential space that is located between the anterior aspect of the vertebral body and the prevertebral fascia. It is located directly posterior to the retropharyngeal space.
Step off: Normally, there is “step off” from the hypopharynx to the larynx. This is due to the soft tissue density of the undistended esophagus posterior to the tracheal air column.
Requirements:
- Neck extension
- End-inspiration
If the patient’s neck is flexed and/or if the radiograph is obtained during end-expiration the prevertebral soft tissues may appear falsely widened and thus give the false impression of a possible retropharyngeal infection.
Approach:
While describing an X-ray in ENT or Otorhinolaryngology, you need to comment on these points:
- Plain or Contrast
- Regions: Mastoid, Nose and PNS or Soft-tissue neck
- View: AP, lateral, other views of mastoid x-rays
- Important anatomical landmarks
- Pathological findings
- Diagnosis
When interpreting an X-ray of soft-tissue neck, never forget to comment on these points:
a. Cervical vertebrae:
- Erosion of vertebral bodies
- Loss of cervical lordosis (due to prevertebral muscle spasm)
b. Pre-vertebral soft tissue shadow:
- Widening: considered to be widened if >3/4 the width of the body of corresponding vertebra
- Contour: should normally follow the contour of anterior aspect of cervical vertebra
- Foreign body
- Air-fluid level
- Gas shadow
c. Epiglottis
d. Air column in subglottic space and trachea
e. Hyoid bone and laryngeal cartilage ossifications
Importance of lateral view of neck:
This view helps in the diagnosis of:
- Foreign bodies of larynx, pharynx and upper oesophagus and to differentiate a foreign body of the airway from that of the food passage.
- Acute epiglottitis (Thumb sign).
- Retropharyngeal abscess.
- Position of tracheostomy tube, T-tube or laryngeal stent.
- Laryngeal stenosis.
- Fractures of larynx and hyoid bone and their displacement.
- Compression of trachea by thyroid or retropharyngeal masses.
- Caries of cervical spine, associated with retropharyngeal abscess or osteophytes in cervical vertebrae or injuries of spine.
Importance of Anteroposterior (AP) view of neck:
- This view is useful to differentiate a foreign body of larynx from that of oesophagus.
- It is also done to see any compression or displacement of trachea by lateral neck masses, e.g. thyroid tumours or enlargement.
Differential diagnoses:
a. Subglottic tracheal narrowing:
- Circumferential: Croup (Common), Subglottic stenosis, Paradoxic collapse with other glottic obstruction
- Asymmetric: Subglottic hemangioma, Post-tracheostomy fibrosis, Intratracheal thyroid, Subglottic mucocele, Histiocytoma, Papilloma, Intratracheal thymus
b. Retropharyngeal soft tissue thickening:
- Common: Buckling of airway (pseudothickening), Inflammation (adenopathy), Retropharyngeal abscess
- Moderately common: Edema with C-spine injury, Retropharyngeal tumor
- Uncommon: Non-inflammatory adenopathy, Osteomyelitis of C-spine, Tumors of C-spine
- Rare: Myxedematous thickening, Edema with SVC obstruction, Vein of Galen aneurysms, Enteric cyst, Goiter
False prevertebral swelling: Lateral oblique view, Neck flexion, Crying
c. Epiglottic and Aryepiglottic fold enlargement:
- Common: Epiglottitis
- Uncommon: Angioneuritic edema, Corrosive burns
- Rare: Face and neck edema, Tumor, Aryepiglottic fold cyst, Sarcoidosis, Hemorrhage (Hemophilia), Radiation
X-ray findings in diseases:
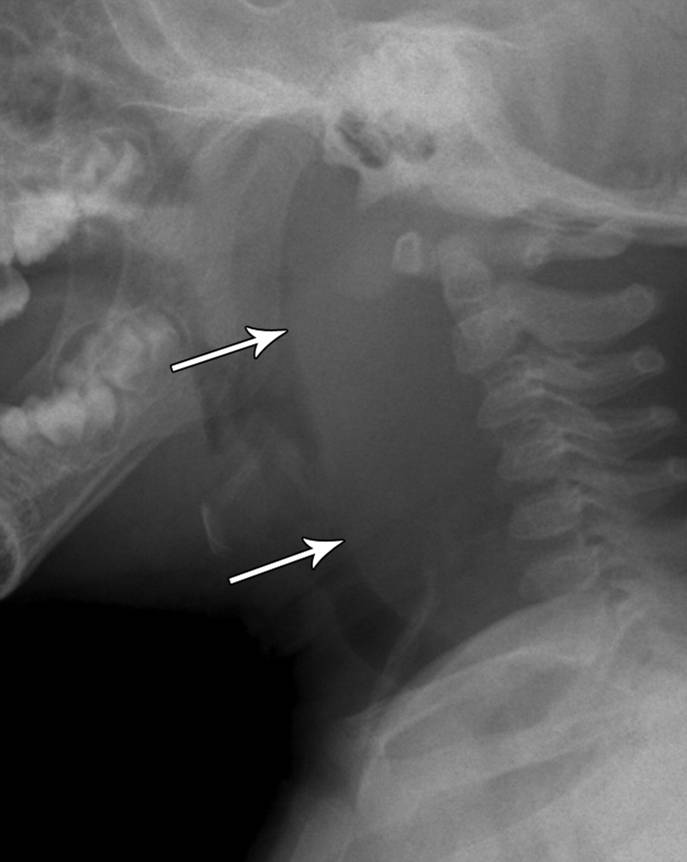
a. Epiglottitis:
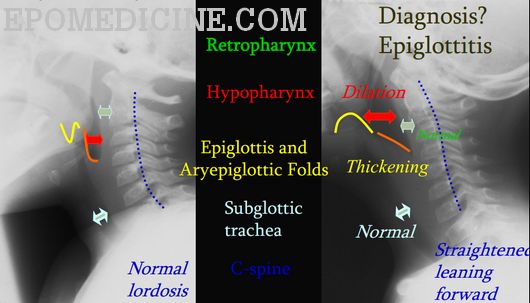
- Enlarged epiglottis (> 8mm) – thumbprint sign
- Loss of vallecular air space
- Thickened aryepiglottic folds (>7 mm)
- Distended hypopharynx
- Straightening of cervical spine
Adult epiglottitis radiographic criteria:
- Epiglottic height-to-width ratio> 0.6
- Epiglottic to C4 vertebral body width ratio > 0.33
- Aryepiglottic fold to C3 vertebral body width ratio > 0.35
- Prevertebral soft-tissue to C4 vertebral body width ratio > 0.25
- Hypopharyngeal airway to C4 vertebral body width ratio > 1.5
b. Retropharyngeal infection (RPI):
- Widened retropharyngeal space:
- Pediatric: C2 – 7 mm and C6 – 14 mm
- Adults: C6 – 22 mm
- Reversal of normal cervical lordosis
- Foreign body
- Air-fluid level
- Gas
c. Croup (Laryngotracheobronchitis):
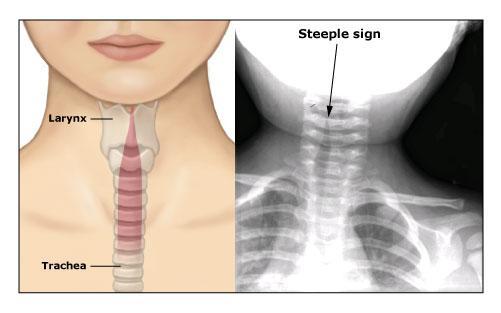
- Subglottic narrowing (Steeple sign)
- Distended hypopharynx
- Subglottic edema
d. Foreign body:
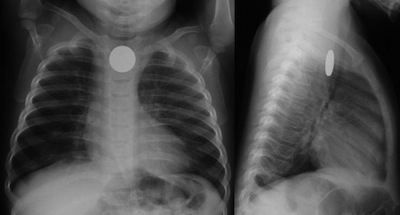
- Visualization of radio-opaque foreign body
- Widened pre-vertebral shadow
- Loss of lordosis
- Location-
- Esophagus: Coronal plane
- Trachea: Sagittal plane (best seen on lateral)