
Jaundice refers to accumulation of bilirubin in the epidermal tissues of the body, resulting in a yellowish tinge to the skin, sclera, and mucosa. Atleast 5 mg/dl of bilirubin level is required for clinically recognizing hyperbilirubinemia.


A) Physiological Neonatal Jaundice:
General consideration:
- In term: peaks (6 to 8 mg/dl) by 3 days of life and then falls
- In preterm: may peak (10 to 12 mg/dl) on 5th day of life
- Newborns who are jaundiced in the first day of life, or who require phototherapy at any point, do not have simple physiologic jaundice.
Causes:
- Bilirubin overproduction: Relative to adults, they have –
- relative polycythemia at birth
- relatively shorter life span of fetal red blood cells (~ 90 days)
- Slower excretion of bilirubin:
- conjugation mechanism is not fully functional at birth (decreased UDPG-T activity)
- increased enterohepatic recirculation (decreased stool output in the first few days of life and lack of normal gut flora in the neonatal intestines)
- decreased uptake (lower levels of lignadins and decreased binding of ligandin) and decreased excretion by liver
B) Pathological Jaundice:
General consideration:
- Onset of jaundice < 24 hr
- Any elevation of serum bilirubin that requires phototherapy
- Increase in serum bilirubin level > 0.5 mg/dl/hr
- >5 mg/dl bilirubin on 1st day of life; >10 mg/dl on 2nd day; >15 mg/dl thereafter
- Persisting beyond 3 weeks
- Conjugated hyperbilirubinemia (dark urine staining nappy)
- Signs of underlying illness: vomiting, lethargy, hyperthermia, hypothermia, tachypnea
Causes:
- Bilirubin overproduction:
- Hemolysis:
- ABO incompatibility, Rh incompatibility
- Congenital hemolytic disease: G6PD deficiency (more common in persons of Asian, African, or Mediterranean descent), RBC membrane defects such as spherocytosis
- Acquired hemolysis: Sepsis, Vitamin K deficiency, Nitrofurantoin, Sulfonamides, Antimalarials, Penicillins
- Extravasated blood: Petechiae, Cephalhematoma, Pulmonary/Cerebral/Occult hemorrhage
- Polycythemia: Infant born to diabetic mothers, LGA, SGA, Delayed cord clamping
- Increased enterohepatic circulation: Pyloric stenosis, Hirschprung disease, Meconium ileus, Intestinal atresia
- Hemolysis:
- Bilirubin undersecretion:
- Conjugation defect or delay: Criggler-Najar syndrome, Gilbert syndrome, Hypothyroidism, Prematurity, UDGP-T variant
- Increased enterohepatic circulation: Inadequate breastfeeding (Breast feeding jaundice), Intestinal obstruction
- Cholestatic jaundice: Biliary atresia, Dubin-Johnson and Rotor syndrome, Choledochal cyst, Cystic fibrosis, Alpha-1 antitrypsin deficiency
HISTORY FOR NEONATAL JAUNDICE
Mnemonics: DEFGhI
- Delivery complications:
- Assisted delivery (forceps/vaccum)
- Delayed cord clamping
- Ethnicity: African, Asian or Mediterranean
- Family history:
- Anemia and jaundice: Spherocytosis, G6PD deficiency
- Liver disease: Galactosemia, Gilbert disease
- Sibling: Rh incompatibility
- Blood group of mother and child
- Gestational history:
- IUGR
- Gestational Diabetes
- TORCH infection
- Maternal use of drugs like sulfonamides (displace bilirubin from albumin and also cause G6PD deficiency hemolysis)
- Input/Output:
- Input: Poor feeding, Exclusive breast feeding
- Output: Poor voiding/stooling ouptut, Color of urine and stool (dark urine and acholic stools in cholestatic jaundice)
Prolonged jaundice: If the jaundice persists beyond 2 weeks in term neonate and beyond 3 weeks in preterm neonate, the cause may be –
- Hypothyroidism
- Biliary atresia
- Hemolytic diseases
- Urinary tract infection
Difference between breast milk and breastfeeding jaundice:
| Breast milk jaundice | Breast feeding jaundice | |
| Onset and Duration | Late onset and Prolonged (>3 wks) | Early onset and resolve by 3 weeks |
| Incidence | 2-4 % | 12-13 % |
| Course | By day 4, instead of usual fall in total serum bilirubin, it may continue to rise and may reach 20-30 mg/dl by 14 days of life. It falls rapidly in 48 hours if breast feeding is stopped. If breast feeding is continued, it stays elevated and slowly falls returning to normal by 4 to 12 weeks. | It appears between 24-72 hours, peaks by 1-2 weeks and disappears by 3rd week. |
| Mechanism | Unidentified factors in milk that inhibit bilirubin metabolism
Ingestion of Beta-glucuronidase of milk and increased enterohepatic circulation |
Decreased intake of milk leading to decreased gut motility and increased enterohepatic circulation |
PHYSICAL EXAMINATION FOR NEONATAL JAUNDICE
- Small or large for gestational age (SGA, LGA)
- Preterm
- Excessive weight loss since birth
- Ruddiness
- Bruising or cephalohematomas
- Hepatosplenomegaly (as a sign of infection, hemolysis, or liver disease)
- Abdominal distention (as a sign of obstruction)
- Vital sign abnormalities (as a sign of infection)
- Omphalitis
- Chorioretinitis (TORCH infection)
- Signs of hypothyroidism
Bilirubin toxicity
2.5 mg of bilirubin will bind tightly with 1 gm of Albumin. Hence, the causes may be –
- Decreased binding of bilirubin to albumin: Prematurity, Free fatty acids, Drugs
- Blood brain barrier disruption: Hyperosmolarity, Anoxia, Hypercarbia, Prematurity
Levels of bilirubin toxicity:
- > 20 mg/dl: In Low Birth Weight (LBW) and Hemolytic disease
- > 25 to 30 mg/dl: In health full-term baby
1. Acute Bilirubin Encephalopathy:
a. Early phase: Hypotonia, Lethargy, High-pitched cry, Poor sucking
b. Intermediate phase: Hypertonia of extensor muscles (opisthotonus, rigidity, oculogyric crisis, retrocollis), Irritability, Fever, Seizures
- Those who survive this phase develop kernicterus
c. Advance phase: Pronounced opisthotonus, shrill cry, apnea, seizures, coma and death
2. Chronic Bilirubin Encephalopathy (Kernicterus):
- Athetosis
- Sensorineural deafness
- Limitation of upward gaze
- Dental dysplasia
- Intellectual deficits
APPROACH TO MANAGEMENT OF NEONATAL JAUNDICE
A. Investigations:
1. Total serum bilirubin (TSB):
Indications are:
- Unsure about visual assessment
- Jaundice in 1st 24 hour of life
- If TcB measurement is > 12-14 mg/dl (beyond 24 hours)
- If mother is Rh negative
2. If bilirubin is > 12 mg/dl and infant is < 24 hours or Mother belongs to Rh-ve blood group:
- Perform Direct Coomb’s test (DCT):
- If positive: Identify antibody (Rh, ABO, Kell)
- If negative or if prolonged jaundice: Look at levels of Direct bilirubin
3. Direct bilirubin level:
- If > 2 mg/dl or > 20% of total bilirubin level: Probably a cholestatic jaundice
- If <2 mg/dl or < 20% of total bilirubin level: Perform Hematocrit
4. Hematocrit:
- High: Polycythemia
- Normal or low: Perform Peripheral Blood Smear (PBS) and reticulocyte count
- Normal: Enclosed hemorrhage, Increased enterohepatic circulation, Hypothyroidism, Gilbert syndrome, Respiratory distress syndrome
- Abnormal: Hemolytic anemia
5. Investigations for cholestatic jaundice:
- Liver function test (LFT)
- Ultrasonography of abdomen: to rule out a choledochal cyst, biliary stones, sludge formation, or tumor compressing the extrahepatic bile duct
- Test for infection: Urine CMV culture (TORCH infection), Urine culture for bacteria, Sepsis screening, Hepatitis A IgM, Hepatitis B sAg
- Alpha-1 antitrypsin level
- Serum and urine aminoacids
- Urinalysis for glucose reducing substance
- Thyroid function test (TFT): TSH, Total and free T4
B. Treatment of Unconjugated Neonatal Jaundice:
1. General measures:
- Early identification of known causes
- Any medication responsible is discontinued/corrected
- Increase feeding volume and calories if inadequate
- Thyroid hormone replacement for hypothyroidism
- If at risk for kernicterus: Exchange transfusion Or Phototherapy Or Phenobarbital
2. Infants with hemolytic disease (including Rh incompatibility):
- Start intensive phototherapy immediately
- If predicted to reach 20 mg/dl – Exchange transfusion
3. Healthy late-preterm and term infants:
Perform visual assessment of jaundice every 12 hourly during initial 3 to 5 days supplemented by Transcutaneous bilirubinometer (TcB) if available. In infants more than 35 weeks gestation, this level should be plotted on an age-specific nomogram to determine the risk level.
Step 1: Does the baby have serious jaundice ?
- Visible jaundice in 1st 24 hours of life
- Yellow palms and soles
- Signs of acute bilirubin encephalopathy or kernicterus
Step 2: If any of the above is present:
- Start phototherapy
- Measure serum bilirubin and determine if baby requires phototherpy/exchange transfusion
- If phototherapy is unsuccessful, other options are – phenobarbital 5-8 mg/kg/day (Crigler-Najjar type II), high dose IVIG i.e. 500-1000 mg/kg over 2-4 hours (for antibody mediated hemolysis), albumin transfusion (binds to bilirubin and prevents crossing BBB), double volume exchange transfusion, oral agar (decrease enterohepatic circulation), metalloporphyrins administration (inhibits heme oxygenase and decrease bilirubin production)
- Determine the cause of jaundice and provide supportive and follow-up care
Step 3: If none of the above is present, continue observation every 12 hours
4. Premature infants: Start phototherapy and exchange transfusion at following levels
| Weight | Phototherapy | Exchange transfusion |
| <1000 gm | Within 24 hours | 10-12 mg/dl |
| 1000-1500 gm | 7-9 mg/dl | 13-15 mg/dl |
| 1500-2000 gm | 10-12 mg/dl | 15-18 mg/dl |
| 2000-2500 gm | 13-15 mg/dl | 18-20 mg/dl |
C. Treatment of Conjugated Neonatal Jaundice:
The stepwise approach to the diagnosis of biliary atresia entails a percutaneous liver biopsy and surgical intervention. If the liver histology is consistent with the diagnosis of biliary atresia, then the surgeon will perform an intraoperative cholangiogram. Intraoperative cholangiogram is considered the gold standard in the diagnosis of biliary atresia, and if the diagnosis is confirmed, the surgeon will proceed with the Kasai portoenterostomy.
PHOTOTHERAPY
1. Mechanism of Action:
- Configurational isomerization/Photo-isomerization (reversible):
- UCB (4Z,15Z) to Isomer (4Z,15E) i.e. Z to E isomer
- Diffuse into blood and excreted into blood without conjugation
- Structural isomerization (Irreversible):
- Converts bilirubin to Lumirubin
- Lumirubin is excreted in bile and urine without conjugation
- Photo-oxidation: Bilirubin is converted into small polar products which are excreted
2. Indications:
- Anticipated rise of bilirubin level to hazardous level
- Prophylactic: Extremely Low Birth Weight (ELBW), severely bruised infants, hemolytic disease of newborn
3. Contraindications:
- Direct hyperbilirubinemia (Bronze baby syndrome)
- Porphyria or family history of prohpyria (Photosensitivity and blistering can be severe)
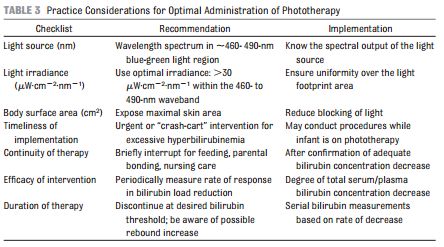
4. Technique:
- Light irradiance: >30 µW/cm²/nm
- Light wavelength: 460 to 490 nm (blue green spectrum). Bilirubin absorbs visible light most strongly in the blue region of the spectrum (460 nm).
- Optimal body surface are: Kept naked except for eyepatches (prolonged exposure to blue light can cause retinal damage in adults) and diaper. Approximately 35% of the total body surface (ventral or dorsal) is exposed. In double photothterapy, infant lies on fibreoptic blankets (biliblankets) with overhead conventional phototherapy (~80% BSA covered)
- Infants are turned every 2 hours
- Distance between baby and light: 30 to 45 cm (can be brought upto 10 cm to maximize effect of phototherapy)
- Monitor:
- Temeprature every 2-4 hours and TSB every 12-24 hours
- Weight daily (Increase 10-20% extra fluids over normal)
- Doscontinue: If 2 TSB values over 12 hour apart fall below cut-offs
5. Adverse effects of phototherapy:
- Insensible water loss
- Watery diarrhea and increased fetal water loss
- Hypocalcemia
- Tanning
- Bronze baby syndrome
- Upsets maternal-infant interactions
EXCHANGE TRANSFUSIONS
1. Mechanism of Action: Removes partially hemolyzed and Antibody-coated RBCs as well as unattached Antibodies and replaces with donor RBCs without sensitizing antigen. With half hour, bilirubin levels return to 60% of pre-exchange level.
2. Indications:
- Phototherapy failure: to prevent a rise in bilirubin to toxic levels
- Hydrops fetalis: to correct anemia and improve heart failure
- In hemolytic disease, immediately if-
- Cord bilirubin > 5 mg/dl and Cord hemoglobin < 10 g/dl
- > 1 mg/dl/hr rise in bilirubin despite phototherapy
- Bilirubin > 20 mg/dl or appears to reach 20 mg/dl
3. Blood:
- Fresh (<7 days old) irradiated reconstituted whole blood (Hct 45 to 50) made from Packed RBCs and FFP
- O negative or Rh compatible with mother and infant
- Double the bolume of infant’s blood (Double volume exchange)
4. Technique:
- Push-pull technique: through umbilical catherter/central venous line
- Isovolumetric exchange transfusion: simultaneously pulling blood out of umbilical arteryand pushing new blood to umbilical vein
- Time: 1 hour
- Phototherapy continued after exchange transfusion
4. Complications:
- Hypocalcemia, hypomagnesemia (CPD blood)
- Hypoglycemia (rebound hypoglycemia)
- Metabolic alkalosis (citrate)
- Hyperkalemia (stored blood)
- Cardiovascular: thromboembolism, arrhythmias, volume overload
- Bleeding disorder
- Infection
- Hemolysis
- Hypothermia or hyperthermia
- Necrotizing enterocolitis