

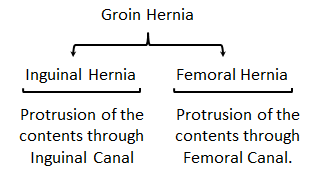
Groin is the area between abdomen and the upper thigh on either sides of pubic symphysis. Protrusions of the abdominal contents through the weak areas in this region are grouped under groin hernias. Groin Hernia can be classified into Inguinal and Femoral Hernias.
Please go though another article of the Hernia Series before reading further:

Relevant Anatomy
Inguinal Region is considered as a weak spot in the lower abdomen owing to the presence of Superficial & Deep Inguinal Ring and the Inguinal Canal. Hesselbach’s Triangle is also considered as a weak spot of the groin through which abdominal contents may protrude is labeled as Direct Inguinal Hernia.

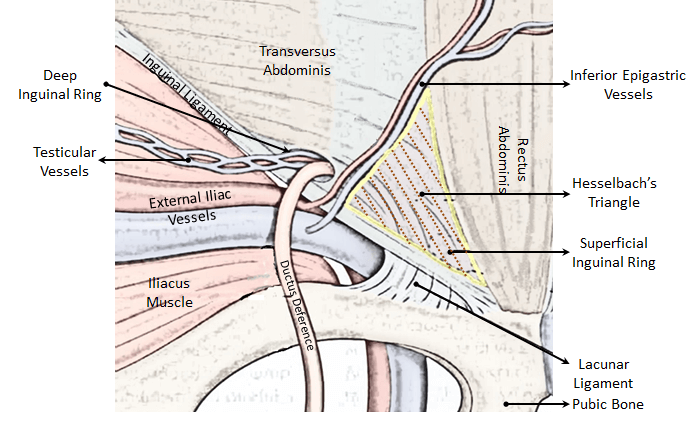
Boundaries of Hesselbach’s triangle
Medial: Rectus Abdominis
Lateral: Inferior Epigastric Vessels
Inferior: Inguinal Ligament
Floor: Fascia Transversalis
Roof: Conjoint tendon
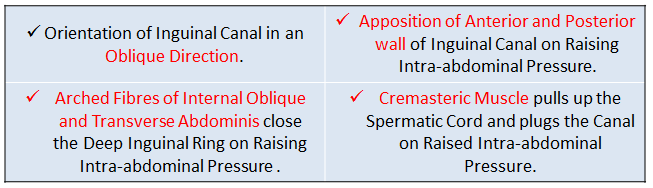
Though the said areas are considered as weak spots, not all humans manifest hernia. Below are the natural mechanisms preventing the occurrence of Inguinal Hernia.

Presenting Features
Hernia manifests in a wide range of symptoms, from a mere swelling to intense pain.
- Lump: Almost all the patients visiting the Surgeon are aware of the Swelling in the Groin.
- Pain: Pain is one of the common complaints from the patients, it is characterized as a vague, dull and dragging worsening by straining, lifting heavy weights and by the day ends. Initially it is low in intensity and gradually as the hernia fully forms, results in a sense of heaviness. It may radiate to the Epigastric Region, if Mesentry is pulled into the Hernia Sac or felt all over the abdomen, if Omentum is pulled.
Once pain becomes intense and becomes unbearable, strangulation or inflammation has to be suspected.
- Gastro-Intestinal Complaints: Vomiting, Constipation, Abdominal Distension and Colicky Pain suggest Intestinal Obstruction.
- Neurovascular Symptoms: Paresthesia due to compression of nerves in the inguinal canal.
- Others: Chronic Lung Diseases leading to Cough, causes of Constipation/Dysuria may be present.
History of previous surgeries has to be noted:
- Appendectomy may injure IlioIngunal Nerve, which later leads to weak abdominal wall.
- Hernia Repair may lead to recurrence.
- Any other Abdominal Surgery may cause Incisional Hernia.
Clinical Examination
Examination is mandatory in order to rule out other possibilities of groin swellings, confirm the diagnosis and to know the progression of the condition.

The Examination of the patient has to be done in both supine and standing position to know the actual size of the hernia.
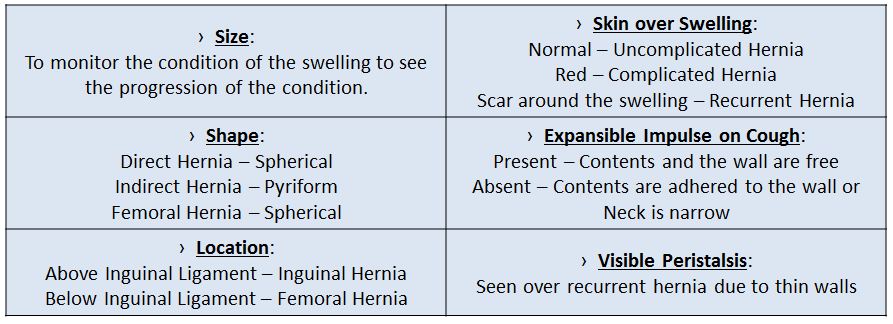
- Appearance: Dimensions of the swelling, colour & character of the skin over the swelling, expansible impulse on cough (or Valsalva) and visibility of peristalsis are to be noted. Abdominal Wall tone is checked by Head and Leg Raising Test by looking for Malgaigine Bulges.

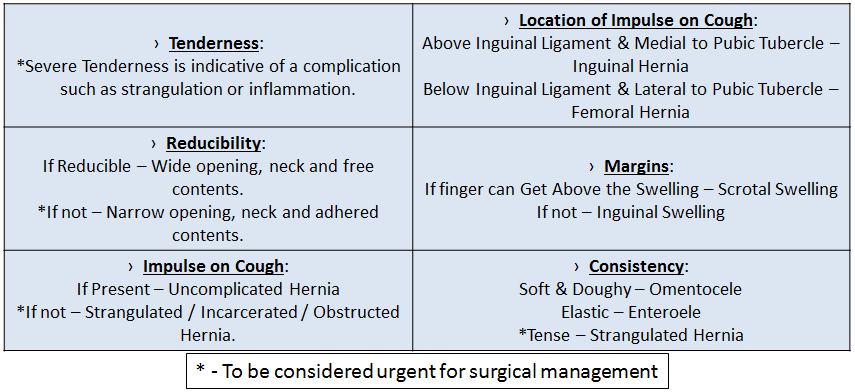
- Palpation: Tenderness and Reducibility of the swelling is checked, impulse on cough is confirmed by placing fingers on Deep, Superficial Inguinal Rings and Femoral Ring. Margins of the swelling are confirmed especially the superior border. Consistency of the swelling is to be determined.



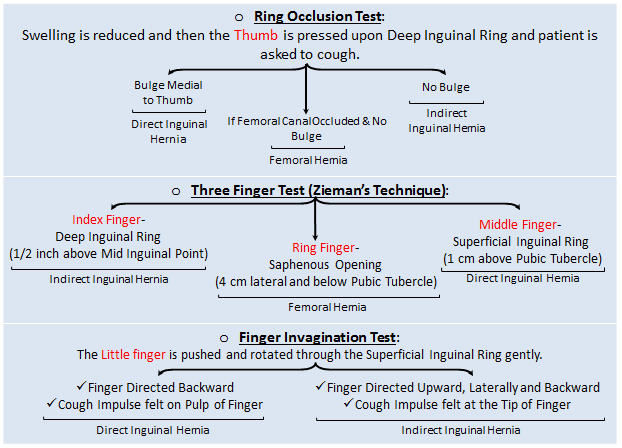
All 5 fingers of ones hand are used in Diagnosing Hernia.
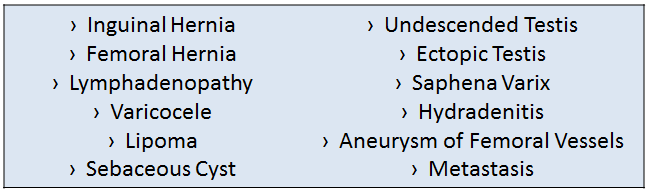
Groin on the other side also needs to be examined to compare. Other Differential Diagnoses have to be ruled out during this phase of examining the patient, such as looking for varicose veins (Saphena Varix), presence of both the testes (Undescended/Ectopic Testis), Slip sign (Lipoma) and presence of Punctum (Sebaceous cyst).
Systemic Examination also has to be done to know the cause of increased Intra-abdominal Pressure such as, Respiratory System, Abdomen, Renal System and Rectum.
Investigations
Diagnostic tests seem to be of very little importance in diagnosis of Hernia, as in most of the situations final diagnosis is approached to by Clinical Examination itself. Investigations can be found useful in the detection of occult Inguinal / Femoral Hernia and in cases of unambiguous diagnosis.
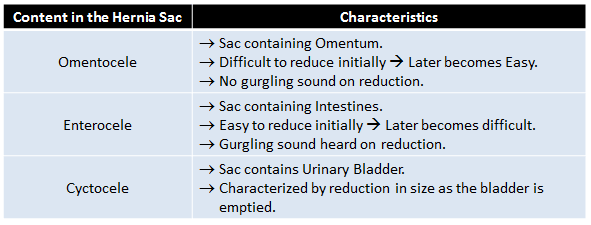
- Ultrasonography: USG is considered as the least invasive and expensive with least exposure to radiation. Bony landmarks and Inferior Epigastric Vessels can be used in differentiating the type of hernia. It can detect the type of content in the sac and its active movement is considered uncomplicated.
- Higher modality of investigation (CT / MRI) is used in reserved cases where USG is inconclusive.

Treatment
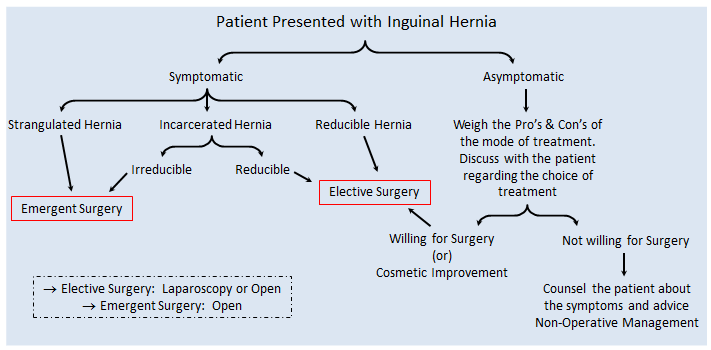
As discussed earlier Hernia may present to the Surgeon in a varied range of situations and an appropriate decision has to be taken regarding the management of the patient after provisionally diagnosing the stage of hernia. All patients with hernia may not require surgery.

Conservative management
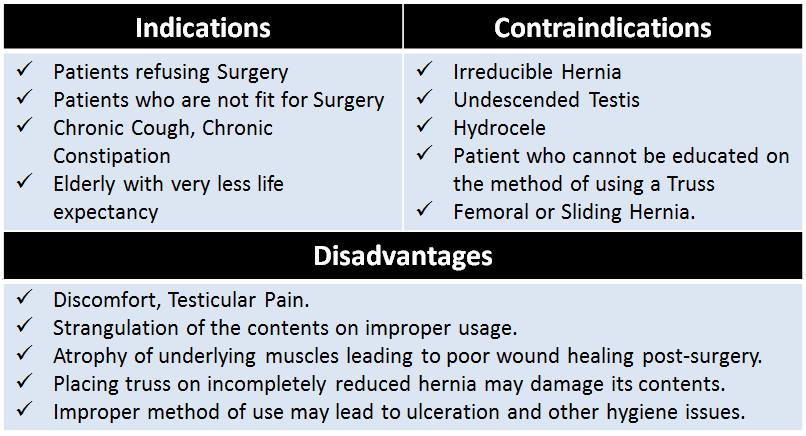
A patient who is asymptomatic and is at a risk of developing complications during Anesthesia or with Chronic Cough or an Elderly should not be advised Surgery, but can be kept under ‘Watchful Waiting’ and should be managed symptomatically. Treatment targets are Pain (Analgesics) and Swelling (Truss).
- Truss: It is considered as a conservative treatment for asymptomatic hernia, where it only prevents the contents of abdomen to protrude out and not a definitive treatment. The prerequisite to using a Truss is that the hernia should be freely reducible. Patient needs to be properly counseled about the method of using it and to maintain hygiene. Truss needs to be applied once the swelling is completely reduced and has to be worn throughout the day except at night.

Surgical Approach to Hernia
Surgery is the only mode of therapy to completely treat Hernia, which has reduced the rates of complications and recurrence over Conservative Management. There are various approaches and methods to repair hernia, but all of them follow the similar basic principles.
- Asepsis
- Reducing the contents of the sac into the abdomen
- Closure of the defect by reconstructing the floor of Inguinal Canal
- Use prosthetic material to reinforce the area of weakness
- Maintain ‘Tension Free’ repair
Preoperative Care:
It should be made sure that conditions such as Chronic Cough, straining during micturition / defecation, ascites and all other conditions leading to increased intra-abdominal pressure have to be treated, if these are not taken care of it may lead to recurrence. General considerations which are taken up before any other surgery remain the same.
Anesthesia :
A variety of methods can be used form Local to General depending on the procedure to be conducted.
- Local Anesthesia – Used in an uncomplicated situation where during surgery the muscles remain in their original tone making tensionless approximation easier.
- General Anesthesia – Conditions with intestinal obstruction need the use of general anesthesia with a cuffed ET Tube to prevent aspiration during manipulation of the bowel in the sac
Elective Surgery
In view of cosmetic improvement or in uncomplicated presentation, the patient is not operated on the day of presentation but at the convenience of both the patient and surgeon.

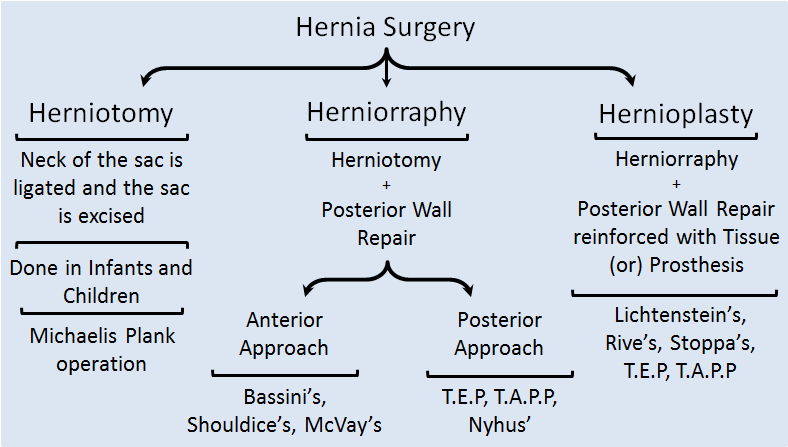
Herniotomy:

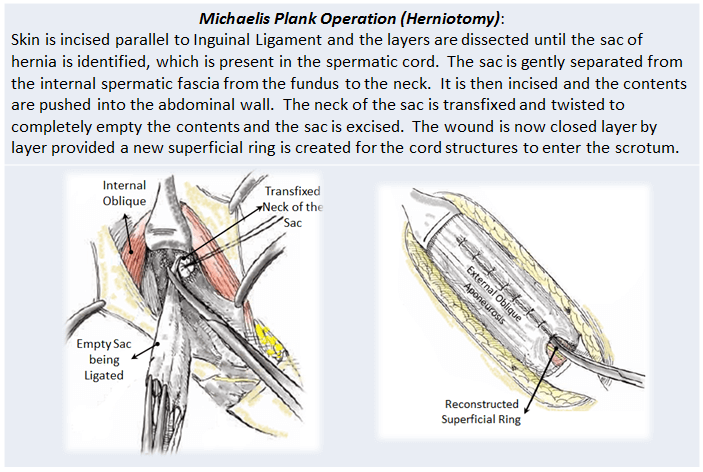
Pictures depicting ligation of the empty sac and reconstruction of the Superficial Ring.
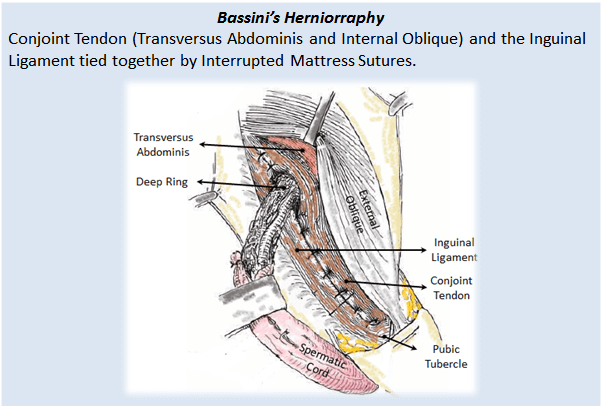
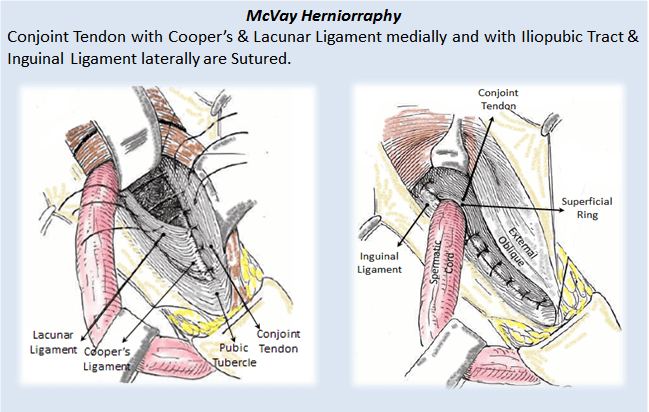
Herniorraphy: The initial steps until excision of the sac are similar to Herniotomy, additionally the posterior wall of the inguinal canal is repaired by sutures and the wound is closed in layers.



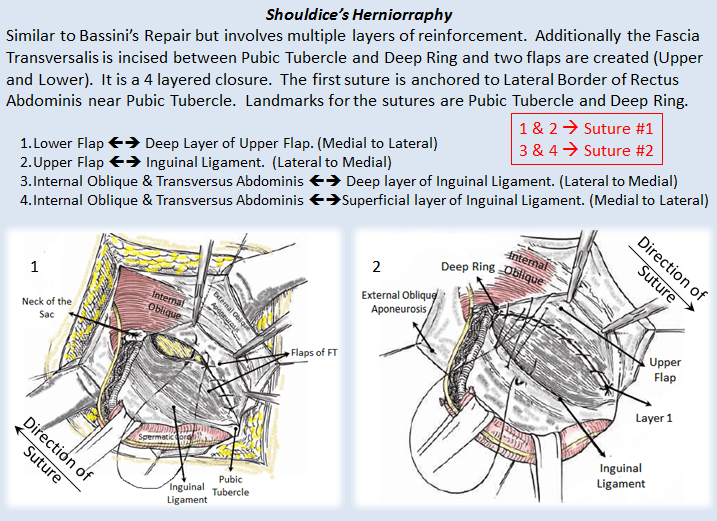

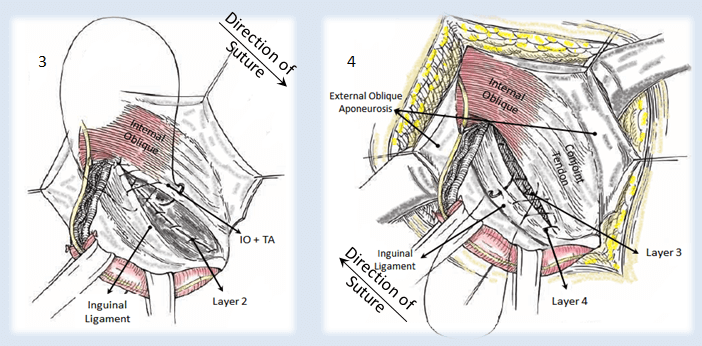
Nyhus’ Herniorraphy is a method where the Transaponeurotic Arch (Transversus Abdominis and Transversalis Fascia) is sutured to Conjont Tendon and Iliopubic Tract.
Hernioplasty: This procedure maintains the principle of Tension-free posterior wall, hence preventing recurrence.

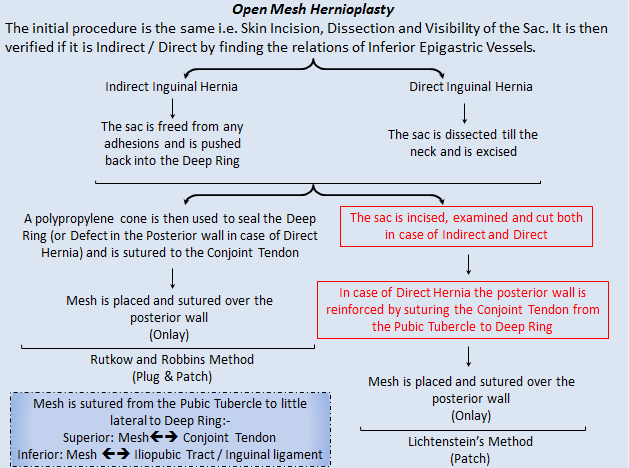
The Mesh used is a Polypropylene Mesh. It is first approximately cut into the appropriate size and a slit is created on the lateral side for the Spermatic Cord and Ilio-inguinal nerve to pass through. The Mesh is positioned 2 cm medial to the Pubic Tubercle till the Anterior Superior Iliac Spine.
The cone is also made of Polypropylene. It is used to seal the defect and is placed under the Conjoint Tendon so as the Pre-peritoneal Fat does not protrude out.
After placing the mesh the wound is closed in layers.

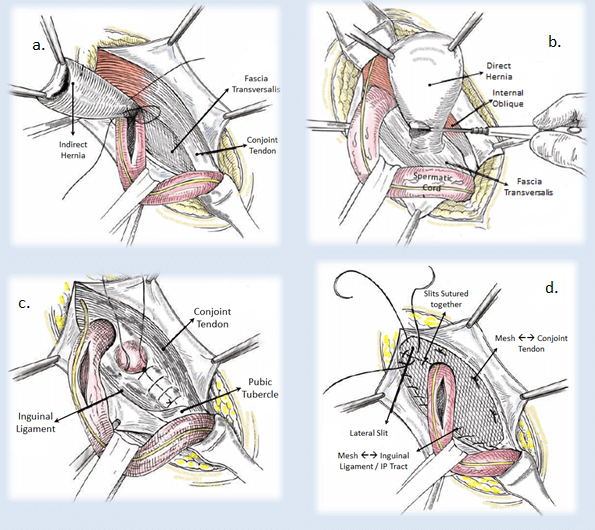
a. Indirect Hernia Sac being inspected before Excision, b. Direct Hernia Sac being Excised,
c. Reinforcement of the Posterior Wall of Inguinal Canal, d. Fixing the Mesh on the Posterior Wall

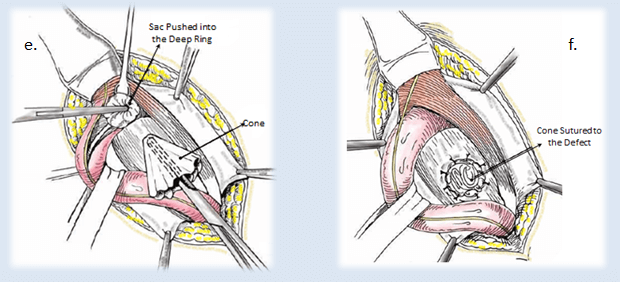
e. & f. Rutkow & Robbins Method (e. Cone being placed into the Deep Ring, f. Cone sutured to the Defect in the Posterior Wall)
Laparoscopic Mesh Hernioplasty: Laparoscopy is gaining advantage over conventional open Hernioplasty owing to reduce pain, faster wound healing, reduced chance of infection, better visualization of anatomy and good chance to repair most of the defects causing hernia. The main types of Laparoscopic procedures done are:- Transabdominal Preperitoneal Approach (TAPP) and Totally Extraperitoneal Approach (TEP).

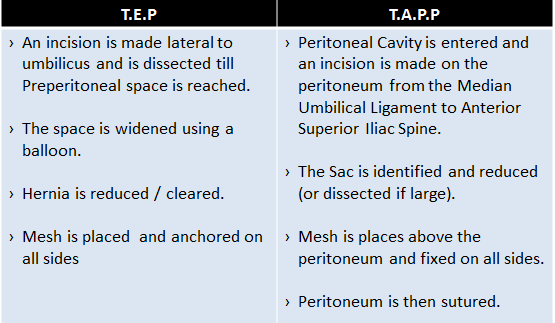
Both the procedures end up placing the mesh in the Pre-peritoneal space but in different methods. During the procedure nerves and vessels are to be taken care of in the Triangle of Pain and Triangle of Doom.

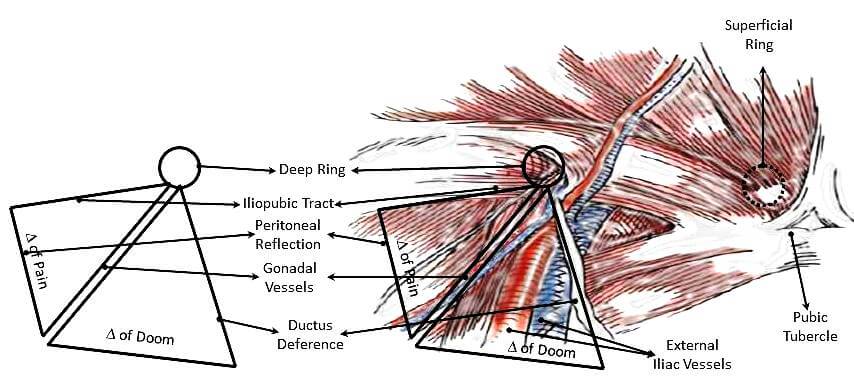
Triangle of Doom – Contains major vessels, if injured may cause a hemorrhagic catastrophe
Triangle of Pain – Contains Femoral Nerve, Lateral Femoral Cutaneous Nerve and Genitofemoral nerve, it is a misnomer (i.e. does not lead to pain). It is just to be cautious of the nerves.

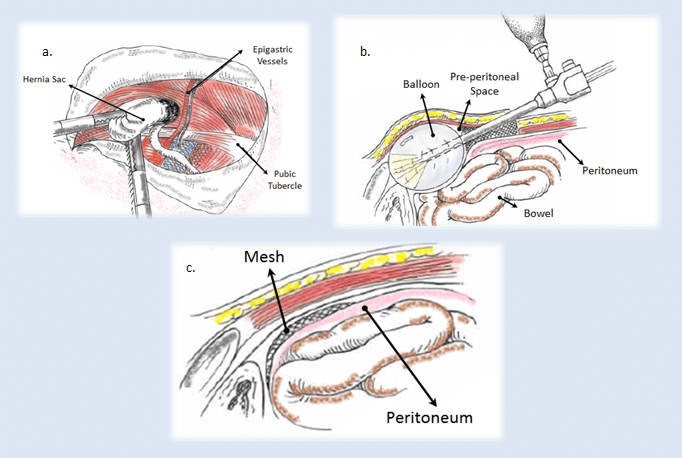
a. Dissection of Sac by TAPP, b. Creating the Pre-peritoneal Space in TEP, c. Final position of Mesh
Stoppa’s Hernioplasty is done in case of very large hernia, recurrent hernias where multiple attempts of repair have shown no positive results or lax abdominal wall, . A large mesh is taken which covers from the Umbilicus to the Pubic Symphysis and horizontally between both the Anterior Superior Iliac Spines (2 cm less than the distance). The mesh is placed by making a midline or Pfanninstiel Incision. The mesh covers whole of lower abdomen and pelvis.
Rives’ Hernioplasty is a Pre-Peritoneal, Transinguinal procedure where the sac is reduced and the mesh is placed above the peritoneum and is sutured to Iliopubic Tract below and Transversus Abdominis above.
Emergency Surgery
In situations such as strangulation or long standing neglected Incarcerated Hernia the patient may suddenly present to the Casualty with severe pain and symptoms of intestinal obstruction an Emergency Hernia Surgery is to be carried out. The patient and the relatives are adequately counseled and all the preoperative precautions (Rehydration and Antibiotics) are taken and an Open Anterior Hernia Surgery is performed. The Sac is opened and the contents are inspected inch by inch and care is taken to prevent any of the contents to drop into the abdominal cavity. Additionally, if the bowel is difficult to examine, the incision may be converted to a Midline Incision. All other principles of surgery are similar to Elective Hernia Surgery and any ischemic or perforated bowel is resected and is anastomosed. Placing the mesh becomes a challenge and is decided on table, to use or not depending on the severity.
Postoperative Care
Most of the surgeries done in the recent times are Day-Care Surgeries where the patient is discharged on the same day. Except in case of emergencies of any intraoperative injury where careful monitoring has to be done.
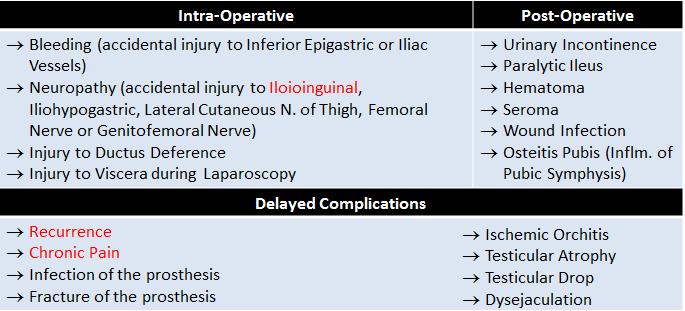
Complications
Hernia repair being a common and easy procedure there are instances of complicated situations arising during the surgery, after surgery or even late after being discharged.

Summary
Hernia is a well known condition in humans since ancient times, which often lead to mortalities owing to the lack of knowledge regarding the anatomy and the mode of treatment. As time passed by, light was shown onto anatomy and many surgeons put efforts on treating the condition.
Hernias in the groin constitute the majority of all, mainly Inguinal Hernia.
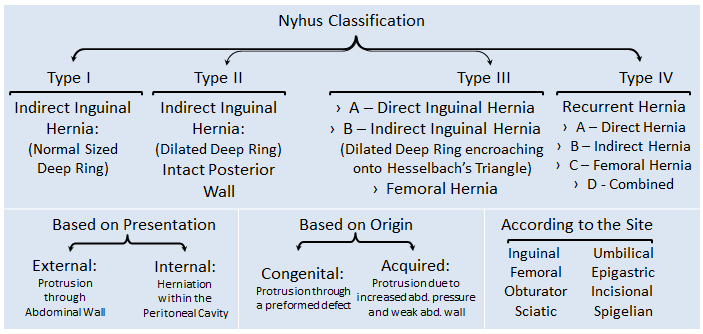
Inguinal hernia is of two types based on the site of origin of the sac, namely Indirect and Direct.
The basic examination is of utmost importance in the diagnosis of Hernia and requirement of any other investigative procedures is very rare.
Once the type of hernia is ascertained, its contents, dimensions and any other complications have to be looked for and surgery followed depends on the Surgeon and is finalized after the patient accepts.
A variety of methods are followed to reduce the contents and reinforce the posterior wall of inguinal canal.
If the patient denies surgery, s/he may be advised conservative management, provided s/he needs to be informed about the symptoms and complications so that visit to the clinic is made at the earliest.
The important complications to be assessed are: Damage to Nerves & Vessels, Spermatic Cord, Viscera and Entrapment of Nerves. Patient needs to be counseled regarding the hygiene needed to be taken at the wound site to avoid future infections.
References
1. Bailey & Love’s Short Practice of Surgery, 27th Edition.
2. Sabiston’s Textbook of Surgery, 20th Edition.
3. S. Das’s Concise Textbook of Surgery, 10th Edition.
4. Schwartz’s Principles of Surgery, 10th Edition.
5. Greenfield’s Surgery Scientific Principles and Practices, 6th Edition.
6. Zollinger’s Atlas of Surgical Operations, 10th Edition.
7. Elsevier Saunders’ Surgical Decision Making, 5th Edition.


Graduated from one of the famous institutions in Telangana, Kamineni Institute of Medical Sciences. He has always been fond of writing articles in Medicine. Since the undergraduate years was interested in making creative Presentations and taking seminars.