


The ear, along the evolution has modified structurally and functionally. In lower animals, they functioned as alarm systems to detect any sounds of the prey or predator so as to fix their vision and also maintain the balance of the body to prevent fall. In the course of evolution, this organ has become a part of the communication.
The ear is divided into 3 parts based on the share of auditory processing:
- External Ear
- Middle Ear
- Inner Ear

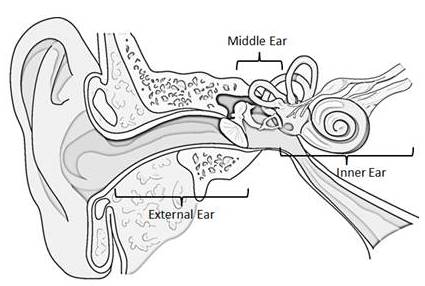
Fig. 1 The Ear
Anatomy of Middle Ear
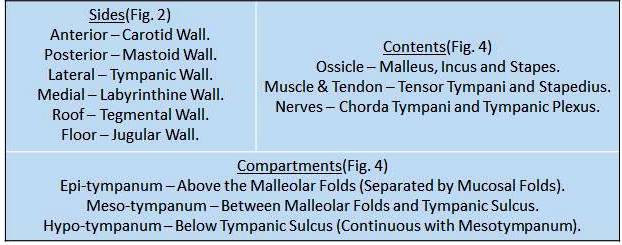
The middle ear is located in the Petrous Part of Temporal Bone. As conventionally considered, it is a 6 sided box.

Fig. 2 Sides of Middle Ear


Boundaries of Middle Ear
Anterior Wall
Divided into 3 parts:
1. Upper – Anterior Epitympanic Sinus (Anterior to Head of Malleus).
Hidden cholesteatoma – remove carefully during surgery (risk of recurrence).
2. Middle – 2 Orifices (from above downward):
- For Tensor Tympani (Muscle)
- For Eustachian Tube
3. Lower – Bone Covering Carotid Artery. It is aThin bone and perforated by:
- Superior and Inferior Caroticotympanic (Sympathetic Nerves around Carotid Artery) Nerves forming Tympanic Plexus.
- Tympanic Arteries (Branches from Carotid Artery)
Lateral Wall (Separates External Ear and Middle Ear)
Formed by: (Above Downward)
1. Scutum – Wedge shaped thin bone in the Epitympanum
2. Tympanic Membrane – Occupies majority of the Wall.
- Pars Tensa: Below Malleolar Folds (Commonly Perforated)
- Pars Flaccida: Above Malleolar Folds (Retraction Pockets)
3. Lateral Wall of Hypotympanum – Thin Bone
4. Chorda Tympani – Explained Later.

Medial Wall (Separates Middle Ear and Inner Ear)
Promontory – Bulge of the Basal Turn of Cochlea.
- On it, are present small groves for Tympanic Plexus.
Oval Window – Behind and Above Promontory.
- Covered by the stapes footplate with its annular ligament.
Round Window –Behind and Below Promontory.
- Covered by Secondary Tympanic Membrane.
Round window is separated from oval window by subiculum (posterior extension of promontory).
Facial Canal – Above Promontory and Oval Window.
- Runs backward till behind oval window and turns downward.
- Bone is thin and can be eroded by a disease in the ear leading to Facial Palsy.
Lateral Semi-Circular Canal Dome – Above Facial Canal at its descent.
Processus Cochleariformis – Above and Anterior to Promontory.
- Corresponds to the Geniculate Ganglion of Facial Nerve.

Posterior Wall
It has lots of surgical importance.
Aditus –An Irregular Opening.
- Located in the Epitympanum.
- Connects epitymapnum and mastoid antrum.
Fossa Incudis –Below Aditus.
- For Short Process of Incus and its ligament.
Pyramid – Below Fossa Incudis.
- Contains Stapedius (Muscle) – attaches to footplate of stapes.
- Connects to the Facial Canal (Containing Nerve to Stapedius).
Facial Canal – Runs downward.
- Contains Facial Nerve.
Facial Recess – Between Pyramid, Facial Canal and Tympanic Annulus
- Canal Wall Up Procedure requires its destruction. It is a procedure in removing cholesteatoma, by leaving the Roof and Posterior Wall Intact.)
Sinus Tympani – Mesotympanum extending posteriorly.
- Lies deep to promontory.
Sinus Tympani is a site for Hidden cholesteatoma – should be carefully cleaned during surgery.

Roof (Separates Middle Ear from Middle Cranial Fossa)
- Represented by Tegmen tympani.
- Formed by Squamous and Petrous parts of Temporal Bone.
- Joined as a Petro-squamosal Suture.
- Veins run in this suture to join the Superior Petrosal Sinus – infections pass into extradural space.
Floor(Separates Middle Ear from Jugular Bulb)
- Represented by a pneumatized or compact bone or rarely as a mucous membrane.
- Entry for the Tympanic Branch of IX Cranial Nerve at the junction of floor and medial wall.
Ear Ossicles
Malleus (Hammer) (Largest of 3 Ossicles)
Head – In Epitympanum.
- Attached to roof by Superior Ligament.
- Facet on the posterior surface for a synovial joint with Incus.
Handle – Runs Downward and Backward.
- Present between the fibrous and mucosal layers of Tympanic Membrane.
- Tensor Tympani attaches to the upper portion.
- Chorda Tympani runs just above this insertion.
Neck – Joins Head and Neck.
- Gives rise to a Lateral process and an Anterior Process.
- Malleolar folds of Tympanic Membrane attach to the lateral process.
Incus (Anvil) (Common to dislocate during Trauma)
Head – In Epitympanum.
- Suspended by Superior Incudal Ligament.
Short Process – Projects Backward into the Fossa Incudis.
Long Process – Projects into the Mesotympanum.
- Tip directed medially and articulates with Stapes
Tip – Also called the Lenticular Process (sometimes refered to as 4th Ossicle)
Incudo Malleolar joint is between Incus and Malleus.
Stapes (Stirrup) (Smallest)
Head – Articulates with the Lenticular process of Incus.
Neck – Stapedius gets inserted.
Crura – Two in number, arise from neck and join the footplate.
Footplate – Placed horizontally over Oval Window.
Incudo-stapedial joint is commonly eroded due to the poor blood supply

Muscles in Middle Ear
Tensor Tympani (Pulls Malleus Medially)
- Arises in the canal above Eustachian tube.
- Turns medially at the Processus Cochlearifoemis and inserts onto the Malleus.
- Supplied by the motor branch of V Cranial Nerve.
Stapedius (Takes off the Foot plate of Stapes over Oval Window)
- Arises from the walls of pyramid on the posterior wall.
- Inserts onto the neck and Posterior Cura.
- Supplied by the branch from VII Cranial Nerve.
Nerves in Middle Ear
Chorda Tympani (Division of CN VII)
- Carries Taste Sensation from the anterior 2/3rd of the same side of the Tongue and Secretomotor fibres to the Sub-Mandibular Gland.
- Runs along the Lateral wall of Middle Ear.
- Enters the ear through the Canal of Huguier in the anterior wall.
- Runs between the Fibrous Layer and Mucosal Layer, initially across the head of the Malleus and then below the Malleolar Folds.
- Reaches the Posterior Wall runs downward till it reaches the Facial Canal.
Tympanic Plexus
- Nerves which innervate the Mucosa of the Middle Ear, Mastoids and Eustachian Tube.
- Lies over the Promontory.
- Arise from the branches of IX Cranial Nerve and Corticotympanic Fibres of Sympathetic Plexus around Carotid.
Blood Supply of Middle Ear
- Arise from External Carotid and Internal Carotid Systems.
- Epitympanum – Branch from Maxillary Artery.
- Mesotympanum and Hypotympanum – Branches from Internal Carotid and Atrery to Pterigoid Canal.
Summary
The Ear, an organ meant for hearing which is essential form communication initially has been designed in animals only for defending themselves by hearing out any threats has evolved to the organ which is today for balance and to complete the circuit of hearing à speaking.
Ear is divided into three parts:- External Ear, Middle Ear and Inner Ear.
External Ear to funnel the sound waves to the tympanic membrane which converts sound waves to mechanical waves. Middle Ear acts as an amplifying and conducting agent. Inner Ear acts as a sensory organ which converts mechanical waves to neural impulses which travel to the hearing centre.
Middle Ear is typically a 6 sided box divided into 3 parts:- Epitympanum, Mesotympanum and Hypotympanum. Anatomy of which has to be kept in mind while operating for various conditions and if interpreted wrong may lead to permanent deafness / loss of facial expression.
References
- Scott – Brown’s Otorhinolaryngology, Head & Neck Surgery.
- Logan Turner’s Diseases of Nose, Throat and Ear Head and Neck Surgery.
- Diseases of Ear, Nose and Throat & Head and Neck Surgery, P.L. Dhingra.


Graduated from one of the famous institutions in Telangana, Kamineni Institute of Medical Sciences. He has always been fond of writing articles in Medicine. Since the undergraduate years was interested in making creative Presentations and taking seminars.