
The anatomy of facial nerve has already been discussed in detail earlier. It is essential to have proper knowledge of anatomy to understand this section of clinical examination of facial nerve.
A) Inspection:
Observe:
- Face at rest for any facial asymmetry
- Any facial tics, symmetry of eye blinking or eye closure
- During smiling
In palsy:
- Blink: The eyelid on the affected side closes just a trace later than the opposite eyelid.
- Nasolabial folds: The weak one is flatter.
- Mouth: The affected side droops and participates manifestly less in speaking.
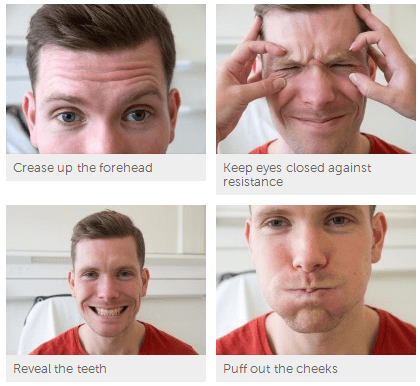
B) Motor function testing:
| Instruction | Muscle tested | Response in palsy |
| Ask the patient to wrinkle his/her forehead | Frontal belly of occipito-frontalis | Asymmetry as he/she cannot wrinkle his forehead on the side of palsy in LMN palsy |
| Ask the patient to close his/her eyes forcibly while you try to open the eyelids with your fingers | Orbicularis oculi | In LMN palsy eyelids don’t close completely. Instead the eyeball rolls up. This is known as Bell’s phenomenon. In healthy individuals, eyelids cannot be opened with mild force against patient’s resistance. |
| Ask the patient to show his/her teeth or smile | Levator anguli oris, Zygomatic major and minor, Depressor anguli oris, Buccinator, Risorius | Angle of mouth deviates towards normal side |
| Ask the patient to blow out cheeks with mouth closed i.e puff the cheeks and assess power by your attempt to deflate the cheekAsk the patient to whistle | Orbicularis oris, Buccinator | Patient can’t blow out his cheek as air escapes from affected side |
| Ask the patient to clench his/her teeth and simultaneously depress the angles of mouth | Platysma | Folds of platysma is seen in the neck as platysma contracts |
C) Sensory function testing (Taste test):
- Explain the procedure to patient and instruct him/her not to speak during the procedure
- Give the patient cards indicating various tests to be tested and instruct him/her to signal by showing the card for the taste perceived
- Ask the patient to protrude out his tongue
- Place sweet, salt, bitter and sour taste solutions on one side of tongue one by one using cotton-bud
- Patient should be asked to rinse his/her mouth after test for each taste
- Test the opposite side also
Other tests (usually not done):
- Corneal reflex (Afferent is by trigeminal nerve while efferent is by facial nerve)
- Schirmer’s test (Secretomotor function)
You may need to:
- Inspect external auditory meatus – Herpes zoster Oticus (Ramsay hunt syndrome)
- Ask if there has been any hearing changes? – facial nerve supplies stapedius – paralysis results in hyperacusis
Differentiating UMN (Supranuclear) and LMN (Nuclear and Infranuclear) Facial nerve palsy:
| UMN type | LMN type | |
| Facial motor function | Wrinkling of forehead preserved (frontalis unaffected) | Total face is involved |
| Bell’s phenomenon | Absent | Present |
| Facial muscles | Not atrophied | Fascicultions, Atrophied |
| Taste sensation | Preserved | May be lost |
| Corneal reflex | Preserved | Lost |
| Hemiplegia | Contralateral | Ipsilateral |
| Babinski reflex | Present | Absent |
Causes of Unilateral and Bilateral Facial Palsy:
1. Unilateral facial palsy: Ramsay hunt syndrome, Acoustic neuroma, Meningioma, Cholesteatoma, Traumatic injury
2. Bilateral facial palsy: Poliomyelitis, Leukemia, Melkersson syndrome, Mobius syndrome, Myasthenia gravis, Myotonic dystrophy
3. Can cause either unilateral or bilateral palsy: Bell’s palsy, Otitis media, Parotid disease, HIV, Leprosy