
Hypertension in pregnancy is one of the major cause of maternal, fetal and neonatal mortality and morbidity in both the developing and developed nations. About 10-15% of pregnancies are accompanied by hypertension and if these are detected early and effective interventions are performed, the prognosis is good.
A. HISTORY FOR HYPERTENSION IN PREGNANCY:
Ask relevant questions necessary to identify the risk factors:
| Maternal general | Age over 40 years |
| Obstetric history | Previous pre-eclampsia |
| Previous gestational hypertension | |
| Multiple pregnancies | |
| Nulliparity or interpregnancy interval greater than 10 years | |
| Artificial insemination with donor sperm | |
| Pre-existing conditions | Chronic hypertension |
| Diabetes mellitus | |
| Congenital heart conditions: coarctation of the aorta, transposition of great vessels, pulmonary atresia with VSD and pulmonary stenosis | |
| Chronic renal disease | |
| Thrombophilia, such as antiphospholipid syndrome | |
| Increased body mass index | |
| Migraine |
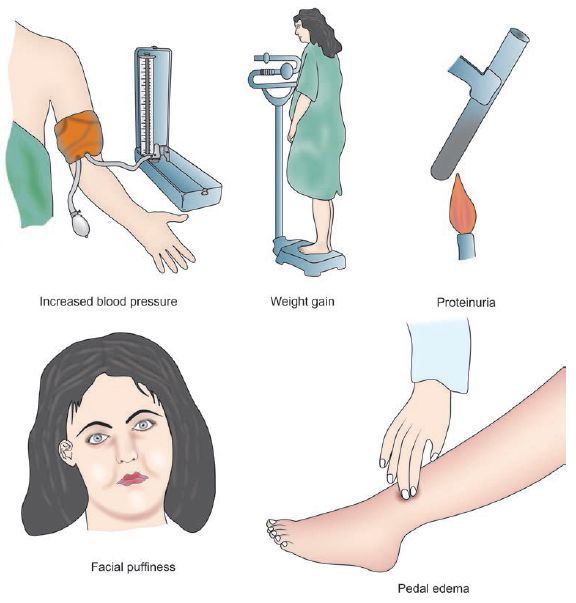
Identify mild and alarming symptoms of hypertension in pregnancy:
1. Mild symptoms (Edema):
This can be due to proteinuria (glomeruloendotheliosis). Since, edema is a universal finding in pregnancy, pathology may be indicated by:
- Persistent ankle edema in the morning
- Tightening of rings on fingers of hand
- Facial puffiness
- Vulval edmea
2. Alarming symptoms:
These alarming symptoms indicate severe pre-eclampsia or it’s complications like eclampsia and end-organ dysfunction:
| Symptoms | Description | Significance |
| Headache | Frontal or Occipital; unrelieved by simple analgesics | Cerebral edema, CNS hemorrhage |
| Visual disturbance | Blurring, diplopia, scotoma | Retinal infarction , Occipital lobe damage (vasogenic edema), Retinal detachment |
| Acute abdominal pain | Epigastric or right upper quadrant; may be associated with vomiting or hematemesis | Hemorrhagic gastritis, Subcapsular hemorrhage in liver, Hepatic necrosis, HELLP syndrome |
| Diminished urine output | Oliguria i.e.<400 ml in 24 hours | Reduced plasma volume (Renal hypoperfusion), Ischemic acute tubular necrosis |
| Dyspnea | Shortness of breath | Acute pulmonary edema, ARDS (Acute Respiratory Distress Syndrome), Penumonia (Aspiration or Infective) |
| Reduced fetal movements | Intrauterine growth restriction (IUGR) or Oligohydramnios | |
| Convulsions or fits What is Status eclampticus?When convulsions occur in quick succession without remission |
1. Premonitory stage (30 seconds): Loss of consciousness, eyeballs roll/turn to one side/fix 2. Tonic stage (30 seconds): Opisthotonus, flexed limb, clenched hands, respiration ceases, tongue protrudes between teeth, cyanosis, fixed eyeballs 3. Clonic stage (1-4 minutes): Generalized twitching starting from face, Tongue bites and blood stained frothy secretions in mouth, Stertorous breathing 4. Stage of coma |
Eclampsia – due to cerebral irritation and excessive release of glutamate (excitatory neurotransmitter) resulting from:1. Cerebral anoxia (vasospasm)2. Cerebral edema
3. Cerebral dysrhythmia |
B. EXAMINATION FOR HYPERTENSION IN PREGNANCY:
1. General Physical Examination:
a. Raised Blood Pressure (Hypertension):
- Position: Avoid measuring blood pressure in supine position lying on back (Supine hypotension syndrome can give false reading)
- Precautions:
- Choose the right size of cuff (encompassing 40% of arm circumference)
- The woman should not use tobacco or caffeine within 30 minutes of the measurement.
- Significant reading: >140/90 mmHg
b. Proteinuria in Dipstick test:
- Qualitative test and not very accurate
- Reagent strip is dipped into fresh urine specimen (first morning specimen is not preferred due to possibility of false high reading) and immediately removed from the specimen
- Assess the color change in reagent strip after 1 minute and compare with the index provided by manufacturer (often on the sides of bottle)
- Grading based on visual assessment: Trace; 1+ = 0.3 g/L; 2+ = 1 g/L; 3+ = 3 g/L; and 4+ = 10g/L
- Significant reading: >1+
c. Edema: Pitting edema localized to especially to the ankle or may be generalized
d. Weight gain: More than 5 lb/month or more than 1 lb/week is significant
e. Signs of pulmonary edema: Crackles, S3 gallop, etc.
f. Petechiae: May indicate HELLP syndrome, Thrombocytopenia, DIC (Disseminated Intravascular Coagulation)
g. Ankle clonus or Hyper-reflexia: Indicates excessive neuromusuclar irritability with possiblity of progression to eclampsia
h. Knee jerks: Reduction or absence is a sign of magnesium toxicity which is used for seizure prophylaxis in severe pre-eclampsia and eclampsia
i. Papilledema (Fundoscopy): Increased ICP associated with malignant hypertension
2. Abdominal examination:
Evidences of chornic placental insufficiency includes:
- Fundal height less than the estimated on the basis of Last Menstrual Period (Intrauterine Growth Restriction or IUGR)
- Uterus may appear full of fetus (Oligohydramnios)
C. DIFFERENTIAL DIAGNOSES FOR HYPERTENSION IN PREGNANCY
On the basis of onset of hypertension, measurement of blood pressure, presence of proteinuria or seizures – establish your provisional diagnosis, which may be:
- Chronic hypertension
- Gestational hypertension
- Pre-eclampsia
- Severe pre-eclampsia
- Eclampsia
- Pre-eclampsia superimposed on Chronic hypertension
Diagnostic criteria and Pathophysiology of Pregnancy induced Hypertension
If a diagnosis of Eclampsia is made, conditions associated with convulsions must be kept in mind, and relevant symptoms and signs must be looked for during history and examination:
- Epilepsy
- Hysteria
- Encephalitis (Perform lumbar puncture if supsected)
- Meningitis (Perform lumbar puncture if suspected)
- Puerperal cerebral thrombosis
- Poisoning (Send urine toxicology if suspected)
- Cerebral malaria
- Intra-cranial tumors (Head CT may be useful)
D. INVESTIGATIONS FOR HYPERTENSION IN PREGNANCY:
| Urinalysis | Proteinuria – dipstick protein of>1+necessitates follow up with a spot urinary protein:creatinine ratio |
| Abnormal is >30 mg/mmol | |
| Full blood count | Haemolytic anaemia |
| Thrombocytopaenia | |
| <100×109/L may indicate DIC | |
| <50×109/L may indicate need for platelet transfusion | |
| Haemolytic anaemia with thrombocytopaenia may indicate HELLP syndrome | |
| Increased Hematocrit (HCt) may indicate decreased plasma volume | |
| Electrolytes and creatinine | Elevated creatinine (>1 mg/dl) |
| Liver function tests | Transaminases>70 IU/L consistent with hepatic parenchymal damage |
| Raised bilirubin from haemolysis | |
| Lactate dehydrogenase | Raised in haemolysis |
| Abnormal coagulation profile | Evidence of DIC (↓ fibrinogen,↑ FDPs) DIC likely in placental abruption, and hepatic subcapsular haematoma |
| Serum urate | > 4.5 mg/dl is a biochemical marker of pre-eclampsia |
| Blood grouping and hold | For RBC and platelet transfusion |
| Fetal assessment | Daily fetal kick count, Ultrasound for oligohydramnios or fetal growth restriction |
| CTG for fetal distress, Umbilical artery flow veolcimetry, Biophysical profile |
E. TREATMENT OF PRE-ECLAMPSIA:
1. Bed rest (Preferably in Left lateral position):
- Increases renal perfusion (diuresis)
- Increases uterine perfusion (improves placental perfusion)
- Reduces blood pressure
2. Diet: Well balanced diet rich in protein (100 gm/day) and calories (1600 kcal/day)
3. Diuretics: Diuretics should be used judiciously as maternal circulatory volume is already reduced. Frusemide (Lasix) oral is indicated for –
- Cardiac failure
- Pulmonary edema
- Diazoxide therapy (associated with fluid retention)
- Massive symptomatic edema
4. Antihypertensive therapy:
a. Short-term control of Blood Pressure (BP): If BP ≥ 160/110 mmHg or MAP ≥ 125 mmHg
| Drug | Dose | Onset | Adverse effects / Comments |
| Labetalol | 10–20 mg IV every 10 min (max. 300 mg) Maintenance: 40 mg/hr |
5 min | It is a combined α and β blocker Bronchospasm in asthmatics, Tremor Heart block |
| Hydralazine | 5 mg IV every 30 min (max. 30 mg) Maintenance: 10 mg/hr |
10 min | It is an arterio-dilator. Hypotension, Palpitations, Lupus like syndrome Neonatal thrombocytopenia |
| Diazoxide | 15–45 mg IV; may be repeated in 5 min (max. 300 mg) |
5 min | It is a Potassium channel opener. Flushing, Hyperglycaemia Tachy- or bradycardia Sodium and water retention |
| Nifedipine | 10–20 mg PO; may be repeated in 30 min (max. 240 mg/24 hr) | 10 min | It is a calcium channel blocker (arterio-dilator) Tachycardia, Flushing, Hypotension, Inhibition of labor Not used in aortic stenosis |
| Nitroglycerine | 5 µg/min IV | 0.5-5 min | Only used when other drugs have failed. It is a venodilator. Tachycardia, headache, Methemoglobinemia Not to be used in hypertensive encephalopathy (↑ICP) |
| Soidum Nitroprusside | 0.25-5 µg/kg/min IV | 0.5-5 min | Only used when other drugs have failed. It is a direct arterial and venous dilator. Severe hypotension, Fetal toxicity (cyanide, thiocyanate) |
b. Oral antihypertensives: For BP falling out of severe level and persistent rise in BP during continued pregnancy or induction of labor
- Oral Methyldopa (Central and peripheral anti-adrenergic): Side effects like Postural hypotension, Postpartum depression
- Oral Nifedipine (Calcium channel blocker): Side effects like edema, dizziness
- Others: Oral Labetolol, Oral Hydralazine
Note: ACE inhibitors and Angiotensin Receptor Blockers (ARBs) are not indicated in pregnancy due to teratogenecity in 1st trimester, fetal renal failure and oligohydramnios.
5. Progress monitoring:
- Daily detailed examination
- Regular weight measurement at weekly intervals
- Daily dipstick test for proteinuria (24 hour estimation if significant)
- Blood pressure measurement to be done every 4 hourly (at least four times a day)
- The following investigation to be done on weekly basis: Hematocrit with platelet count, RFT (blood urea; serum uric acid; and serum creatinine); LFT (AST, ALT and LDH) and ophthalmoscopic examination.
F. TREATMENT OF ECLAMPSIA:
- Maintain Airway, Breathing and Circulation
- Left lateral decubitus position (reduces pressure on Inferior venacava, enhancing cardiac and renal output)
- Suction oropharynx, Protect from injury, Avoid restraining the patient
- Arrest convulsions with Magnesium sulfate regimen (Use phenytoin if contraindication to MgSO4 are present)
- Add IV antihypertensives (Hydralzine or labetalol or calcium channel blockers or nitroglycerine) if BP remains > 160/110 mmHg (Hypertensive crisis)
- Fluid managment:
- Ringer Lactate not exceeding 2 L in 24 hours
- IV frusemide 40 mg only in cases of acute pulmonary edema
- For status eclampticus: Thiopentone sodium 0.5 gm dissolved in 20 ml of 5% dextrose given IV very slowly
- Intubate for airway protection/hypoxia or if seizures refractory to intervention
- Organize investigations
- Delivery of baby (only definitive treatment): No expectant management is recommended regardless of gestational age and must be performed within 6-8 hours if fits are not controlled
- Induction of vaginal delivery is recommended
- Artificial Rupture of Membrane (ARM)
- Oxytocin
- If fits is controlled and cervix is unripe: PGE2 (Dinoprostone) gel can be used
- Cesarean section is indicated if:
- Uncontrolled fits despite of therapy
- Unconscious patient and poor prospect of vaginal delivery
- Obstetric indications
- Women often go into spontaneous labor after onset of seizures, and/or have a shorter duration of labor
- Induction of vaginal delivery is recommended
- Intrapartum monitoring:
- Vitals are recorded half hourly
- Urine output, respiratory rate and Deep tendon reflex for Magnesium toxicity
- Fetal heart rate
G. EARLY POSTPARTUM MANAGEMENT FOR HYPERTENSION IN PREGNANCY:
- Postpartum hemorrhage (PPH) prophylaxis
- Continue MgSO4 as discussed in the regimen
- Neonatal care till mother is stable
- Titration of antihypertensive agents
- Prophylactic antibiotics
Submitted by: Sulabh Shrestha
This article is only for academic purpose and should not be used as a medical advice.