
Synonyms: Spinal tap
Definition: Puncture of subarachnoid space in the lumbar region of the spinal cord to withdraw cerebrospinal fluid (CSF) for diagnostic or therapeutic purpose or inject drugs for anesthetic purpose.
Indications:
A. Diagnostic:
- CNS infections: Bacterial, viral, fungal, parasitic or TB meningitis
- Subarachnoid hemorrhage
- Carcinomatosis meningitis (CNS involvement in leukemia)
- Inflammatory conditions: Multiple sclerosis, Devic disease
- Measuring CSF protein level in Gullian Barre syndrome
- Pseudotumor cerebri
- Monitor efficacy of treatment in presence of CNS infection
- Instillation of contrast material for myelography
B. Therapeutic:
- Intrathecal chemotherapy (methotrexate, cytarabine)
- Inject immunoglobuins (tetanus immunoglobulin)
- Removal of CSF in pseudotumor cerebri (idiopathic intracranial hypertension)
C. Anesthetic:
- Spinal anesthesia for lower limb/lower abdomen surgery
Contraindications:
- Patient refusal
- Uncorrected bleeding diasthesis (risk of epidural hematoma causing cord compression)
- Raised Intracranial pressure (risk of ‘coning’)
- Local infection at injection site (risk of epidural abscess or meningitis)
- Gross lumboscaral anomaly
- Systemic sepsis (risk of epidural abscess or meningitis)
Lumbar puncture or Spinal needle:
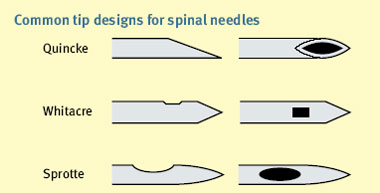
Small diameter (usually 25 G) pencil-point needle such as the Sporette or Whitacre is used. It is thought that the incidence of Postdural puncture headache (PDPH) is higher with Quincke tip because it tends to cut the longitudinal fibres of the dura, whereas pencil-point needles divide the fibres which can reseal later.
There’s color coding for the lumbar puncture needle and purple is the smallest one.
Equipments required:
- Sterile gloves and gowns
- Sterile pack – with gauze, galley pot
- Sterile drapes
- Clorhexidine/betadine in spirit
- Lidocaine 1%
- 5 ml syringe
- 25 G needle (orange)
- Spinal needle
- Manometer
- Three way tap
- Collection tubes: 3 sterile universal containers + glucose tube (fluoride/grey top)
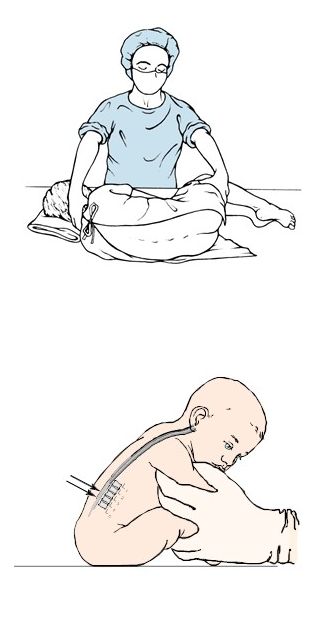
A. Lateral decubitus or Fetal posture: Neck flexed, knees drawn upward towards the abdomen and the back placed to the edge of the table
B. Sitting position: Sitting and bending forward
Site of lumbar puncture:
The spinal cord terminates at the level of L1/L2 in adults and L3 in in infants. Tuffier’s line or Intercristal line is the imaginary line connecting to iliac crests and generally corresponds with the 4th lumbar vertebrae (L4).
Lumbar puncture is usually done at the level of L3-L4 or L4-L5 interspace.
Procedure:
1. Rule out raised ICP:
- History and examination: Cushing’s triad i.e. Hypertension, Bradycardia and Irregular respiration
- Fundus examination: Papilledema
- CT scan of head
2. Clean and drape the site: Identify the desired site of lumbar puncture; clean the area with spirit, povidone-iodine followed by spirit. Drape the area with sterile linen.
3. Local anesthesia: Skin and underlying tissue may be anesthetized with a local anesthesia
4. Introduce spinal needle with stylet: Perpendicular to back – aimed towards the umbilicus and directed slightly cephalad (a sudden loss of resistance of give in will be felt as the needle penetrates duramater)
5. Check for presence of CSF: Remove stylet frequently as the needle is advanced slowly to determine whether the CSF is present.
6. Measure opening pressure: Using a manometer
7. Collect 5-10 ml CSF: 8-10 drops in each vial for microbiological, biochemical and pathological investigation or other relevant investigations as deemed necessary.
8. Instruction: Patient must be kept in horizontal position to avoid lumbar puncture headache.
Complications:
- Cardio-respiratory arrest
- Transtentorial or cerebellar herniation
- Post-lumbar puncture headache
- Introduction of infection
- Spinal cord hematoma
- Intraspinal dermoid formation
- Nerve injuries
Structures penetrated by a spinal needle (Out to in):
- skin
- subcutaneous connective tissue
- supraspinous ligament
- interspinous ligament
- ligamentum flavum
- epidural space
- dura mater (dural sac)
- subarachnoid space (lumbar cistern with CSF)
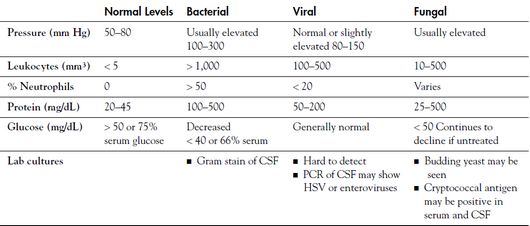
CSF analysis:
- Appearance
- Complete and differential cell count
- Gram stain and bacterial, fungal, and mycobacterial cultures
- Cytology and wet mount inspection
- Spectophotometer analysis for xanthochromia
- IgG and albumin levels, serum IgG and albumin levels to determine the IgG index i.e. (CSF IgG/CSF albumin)/(Serum IgG/Serum albumin)
- Oligoclonal bands
- PCR test for HSV, VZV, EBV, CMV, enterovirus, TB, arbovirus, toxoplasmosis
- Other test for pathogens including syphilis (VDRL or FTA-ABS), cysticercosis, histoplasmosis, coccidiodomycosis, malaria
CSF analysis in Neonates:
