The anatomical basis of Upper Motor Neuron Lesion (UMNL) has already been discussed earlier. Similarly, we will explain the anatomical basis of clinical syndrome of Lower Motor Neuron Lesion (LMNL).
A. Ipsilateral involvment:
- Lower motor neuron comprises of motor neurons in the anterior neurons and the fibers originating from them, which innervates the skeletal muscles.
- These fibers go uncrossed to the same side.
B. Involvement at the level of lesion:
- Damage of LMN at the level of lesion.
C. Flaccid paralysis, Loss of Deep Tendon Reflexes and Hypotonia:
In voluntary muscle contraction: UMN → LMN
In reflex muscle contraction: Muscle sensory neuron → LMN
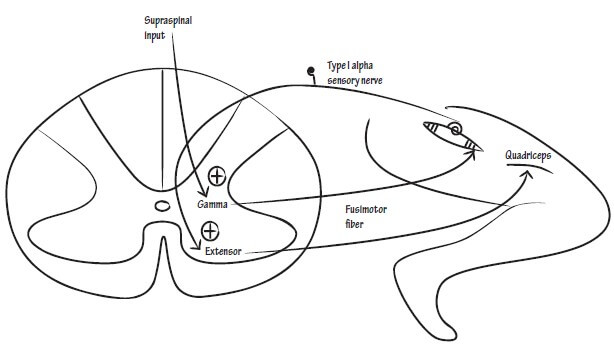
Tone: γ efferent → Regulates baseline Ia afferent discharge → Regulates baseline α-motor neuron discharge
- Alpha motor neurons and axons from them activate extrafusal fibers and contract them.
- So, destruction of this leads to:
- Loss of efferent limb in monosynaptic stretch or deep tendon reflexes
- Information from motor cortex doesn’t reach muscles due to defect in Lower motor neuron – leading to flaccid paralysis
- Loss of gamma and alpha motor neurons lead to decrease in baseline Ia and alpha motor neuron discharge – leading to hypotonicity
D. Muscle atrophy:
- Denervation (deprived of necessary trophic factors)
- Disuse
E. Fasciculations and Fibrillations:
- Damaged α-motor neuron → Spontaneous action potential → Motor unit fires → Visible twitching of muscle fibers group (fasciculations)
- Increased excitability of muscle fibers due to denervation → Spontaneous contraction of single muscle fiber visible in EMG (fibrillations)