Start examination of patient using WIPER.
- Exposure: Above elbows
- Examine both hands side by side
Learn the general principles of orthopedic examination before you proceed to wrist examination.
Look
Both dorsal and palmar aspects of wrist.
Follow SEADS
Some important points:
- Rheumatoid hand
- Shoulder sign: Outline of thumb will form a step if subluxation of CMC joint >2-3 mm
- Radial malunion: radial shortening and prominence of ulna
- Madelung’s deformity: volar bowing of distal radius with dorsal prominence of ulna
- Dorsal wrist ganglion: overlie scapholunate ligament; just distal to Lister’s tubercle
- Carpal boss (bony swelling at 2nd & 3rd CMC level): more distal than simple ganglion
- Extensor digitorum brevis manus (accessory muscle): distal to extensor retinaculum (moves with finger extension)
- Volar ganglion
Feel
Follow TEST Areas
Areas of emphasis: Follow a sequence (Start dorsal-radial and move in a circle around wrist) –
a. Dorsal:
- Thumb CMC (1st metacarpal base and trapezium)
- Anatomical snuff box (between EPB/APL, i.e. 1st extensor compartment and EPL): Scaphoid in floor
- Radial styloid
- Just proximal to radial styloid: DeQuervain’s tenosynovitis
- 1-2 cm proximal to radial styloid: Superficial branch of radial nerve
- Distal radius
- Lister’s tubercle
- Radial side: ECRL and ECRB (2nd extensor compartment)
- Ulnar side: EPL (3rd extensor compartment)
- 5 cm proximal to radial styloid: Intersection syndrome (intersection of 1st and 2nd extensor compartment)
- Scapholunate interval:
- Lunate: just distal to dorsal rim of radius in line with 3rd metacarpal
- Scapholunate interval: valley between dorsal pole of lunate and proximal pole of scaphoid
- DRUJ
- 4th (EDC and EIP) and 5th (EDM) extensor compartments
- TFCC
- Ulnar styloid
- Ulnar snuffbox (between ECU and FCU)
- Fovea (TFCC): between ulnar styloid and pisiform
- Clinical ulnar variance: measured between ulnar styloid (opposed to articular surface in true ulnar variance) and radial styloid (radial styloid is slightly distal than ulnar styloid normally)
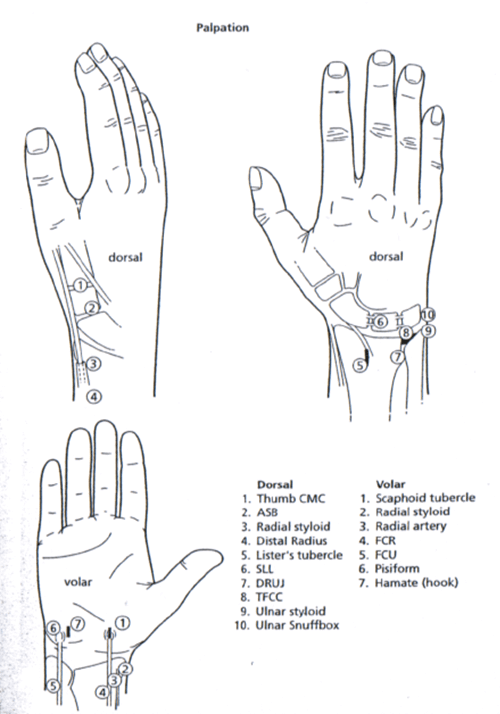
b. Volar:
- Scaphoid tubercle
- Radial styloid
- Radial artery
- FCR
- Palmaris longus and carpal tunnel
- FCU
- Pisiform: within tendon of FCU
- Hamate (hook): slightly distal and radial to the pisiform bone
Move
Test passive then active movements.
- Dorsiflexion: 0-70 degrees
- Palmar flexion: 0-80 degrees
- Radial deviation: 0-20 degrees
- Ulnar deviation: 0-30 degrees
- Pronation: 75 degrees
- Supination: 80 degrees
Measure
Measure grip strength using:
- Dynamometer or
- Sphygmomanometer: First, the sphygmomanometer is rolled into a cylinder comfortable for the patient to grip at rest. The cuff is then inflated to 20 mmHg, and the patient applies maximal grip force to the cuff. The gauge needle indicates the patient’s applied pressure (must increase by at least 150 mmHg).
Neurovascular examination
Test the muscles and nerves. Do not forget to perform Allen’s test.
Modified Allen’s test:
- Ask patient to clench fist and the examiner occludes ulnar and radial artery.
- Patient is asked to release fist after 30 seconds.
- Hand should remain blanched (if not, the pressure applied by examiner is inadequate).
- Release occlusion of ulnar artery to check ulnar artery and radial artery to check radial artery.
- Hand must flush within 5-15 seconds.
Special tests
| Condition | Main site | Test | Technique and Interpretation |
| De Quervain’s disease | Radial | Finkelstein | 1st: Ask to ulnar deviate wrist actively 2nd: Then passively tuck thumb in fist |
| Eichoff’s | Ask to actively tuck thumb in fist and passively ulnar deviate wrist | ||
| Intersection syndrome | Radial | Resisted wrist extension and thumb extension | Increased pain over intersection site |
| Scapholunate instability | Radial | Scaphoid shift test (Kirk-Watson) | Examiner places index finger over SL interval and thumb presses over scaphoid tubercle. With another hand, the wrist is deviated from ulnar into radial deviation. The thumb pressure over scaphoid tubercle resists palmar deviation of scaphoid during radial deviation, which would lead to dorsal subluxation of scaphoid over distal radius dorsal lip in SL instability (“click”). It is positive in upto 36% of normal individuals (esp. with laxity) |
| Midcarpal instability | Central | Midcarpal shift test (Lichtman) | Examiner stabilizes forearm with one hand. With other hand, examiner puts thumb over capitate dorsally. A volar directed force is applied as the wrist is ulnar deviated. A palpable clunk is felt (catch-up movement of proximal carpal row which is slow to dorsiflex in midcarpal instability as the wrist is ulnar deviated) |
| Ulnar sided pathology – general | Ulnar | Ulnocarpal stress test | Axial load to the wrist held in ulnar deviation and neutral flexion/extension. The forearm is then rotated. A positive test elicits pain on the ulnar side of the wrist. |
| Lunotriquetral instability | Ulnar | Ballottement test (Reagan) | Thumb and index finger of one hand fixes lunate. Triquetrum is displaced with thumb and index finger of another hand into dorsal and volar direction. Positive test is indicated by laxity, pain or crepitus. |
| Kleinman Shear test (Shuck test) | Stabilize by pinching lunate with one hand. Apply shear to lunotriquetral joint by applying force on pisiform volarly to push it dorsally (indirect shear on lunotriquetral through piso-triquetral joint). Pain or clicking indicates positive test. | ||
| Pisotriquetral arthritis | Ulnar | Pisotriquetral Grind test | Pisiform is held between the thumb and index finger. Compression is applied and the pisiform displaced back and forth in a radial and ulnar direction. |
| DRUJ | Ulnar | DRUJ Compression test | The examiner compresses the radial and ulnar heads together and then rotates the forearm. |
| Piano key test | Stabilize the forearm and press the ulna with thumb. Increased excursion suggests dorsal subluxation of ulna. | ||
| Radioulnar drawer test | Radius is stabilised with one hand. The ulna is grasped between the fingers and thumb of the other hand and moved dorsally and volarly. | ||
| Dimple sign | Longitudinal traction is applied across the wrist. A force is applied to the dorsal aspect of the ulna shaft. If a ‘dimple’ appears at the level of the DRUJ, then this suggests volar subluxation. | ||
| TFCC | Ulnar | TFCC Compression test | With elbow flexed and rested on table, stabilize forearm with one hand and grasp the fingers with other hand. Wrist is loaded and moved in radial and ulnar deviation. |
| TFCC grind test | Wrist dorsiflexion, axial load, ulnar deviation, and rotation. Pain and crepitus are elicited. | ||
| ECU subluxation | Ulnar | Supination, ulnar deviation and dorsiflexion | Painful subluxation of ECU |
References:
Denby K, Nelson G, Estrada CA. Bedside hand grip assessment with the sphygmomanometer. J Gen Intern Med. 2013 Oct;28(10):1381. doi: 10.1007/s11606-013-2426-0. Epub 2013 Apr 9. PMID: 23568188; PMCID: PMC3785662.